
Abstract
BACKGROUND AND PURPOSE: Head and neck infantile hemangiomas are common lesions that are rarely observed in an intracranial location. We report 4 patients with orbital infantile hemangiomas and ipsilateral enhancing intracranial lesions, presumed to be infantile hemangiomas.
METHODS: Imaging studies and medical records of 4 infants with orbital hemangiomas and enhancing intracranial lesions were reviewed. The intracranial lesions were evaluated in terms of their location, signal intensity characteristics, enhancement pattern, and degree of involution following treatment. Additional findings associated with PHACE syndrome were also noted and a literature review of intracranial infantile hemangiomas and PHACE syndrome was also performed.
RESULTS: The intracranial masses were primarily in or adjacent to the internal auditory canal and demonstrated imaging characteristics and treatment response similar to the ipsilateral orbital lesions. Ipsilateral internal carotid artery hypoplasia, ipsilateral cerebellar hemisphere hypoplasia, and/or other head and neck hemangiomas were present in all patients.
CONCLUSION: These cases collectively support the diagnosis of intracranial infantile hemangiomas and suggest a unique radiographic association between PHACE syndrome and intracranial infantile hemangiomas.
Although infantile hemangiomas are a common head and neck lesion in children, their occurrence in an intracranial location is extremely rare.1-7 The few previously reported intracranial enhancing masses presumed to be infantile hemangiomas have nearly all been associated with concomitant periorbital hemangiomas and PHACE syndrome, which is a rare and heterogenous neurocutaneous disorder with a spectrum of clinical findings that include posterior fossa malformations (P), facial hemangiomas (H), arterial anomalies (A), cardiac anomalies/aortic coarctation (C), and eye abnormalities (E).8 More recent authors also include sternal defects and refer to the syndrome as PHACES syndrome.4 A small number of reported cases of presumed intracranial infantile hemangiomas have been associated with multiple other hemangiomas, including visceral lesions, having been termed “diffuse neonatal hemangiomatosis”.1,7 We present with imaging studies an additional 4 cases of patients with periorbital infantile hemangiomas and concomitant intracranial enhancing masses both before and after treatment with steroids. These cases exhibit characteristic involution of these enhancing masses following treatment, as well as other findings associated with PHACE syndrome, thus reinforcing the association of intracranial infantile hemangiomas with PHACE syndrome.
Methods
Institutional review board approval was obtained for this study. Imaging studies, including CT and MR imaging (MRI), of 4 patients with large periorbital infantile hemangiomas and concomitant intracranial enhancing masses were reviewed from 2 institutions. Review of the studies obtained at presentation revealed additional intracranial abnormalities previously described as part of the PHACE syndrome, including ipsilateral internal carotid hypoplasia, ipsilateral cerebellar hemisphere hypoplasia, and other head and neck infantile hemangiomas. Analysis of the intracranial enhancing lesions was then performed, including the location and imaging characteristics of lesions. The signal intensity of the masses was subjectively compared with the signal intensity of the periorbital hemangiomas on T1, T2, and postgadolinium sequences, and the presence or absence of flow voids was noted.
Repeat imaging studies of each patient following intralesional (n = 2) or oral (n = 2) administration of steroids were also reviewed. The follow-up studies were performed variably between 4 and 42 weeks after steroid administration with an average period of 16 weeks (4, 8, 12, and 42 weeks). Similar analysis of the signal intensity and degree of enhancement of the masses was performed, comparing the masses directly with the periorbital hemangiomas. Additionally, the degree of involution of the masses was estimated with 3D measurements and was compared with a similar measure of the involution of the periorbital hemangiomas.
The clinical records of the 4 patients were obtained and the neurologic and vascular examination findings were reviewed. No other ancillary diagnostic tests were identified, given the relative healthy state of the patients. A review of the literature was then undertaken to better determine the association of the observed findings and the incidence of presumed intracranial infantile hemangiomas both with and without PHACE syndrome. Case reports, research articles, and review articles concerning PHACE syndrome and intracranial infantile hemangiomas from the past 25 years were included.
Results
All 4 patients were female and presented within the first 8 weeks of life for ophthalmologic and radiologic evaluation of large periorbital hemangiomas, 3 right-sided and 1 left-sided (Table). Three lesions were present to some degree at birth with subsequent enlargement, and the fourth lesion appeared shortly after birth as an area of bruising on the eyelid that quickly enlarged.
Summary of clinical and imaging findings
The orbital lesions were significant in each case in that they compromised lid opening and eye movement and posed potential visual complications, including light-deprivation amblyopia and astigmatism. Initial imaging occurred within 1 or 2 weeks following clinical presentation in all cases, with imaging being performed at 3 weeks of age in 2 cases, and at 6 and 8 weeks of age in the others. Three patients were initially evaluated with contrast-enhanced MRI, and the fourth was imaged with contrast-enhanced CT.
All 4 patients were found to have variable degrees of postseptal extension of the periorbital hemangiomas with mild displacement of the globe (Fig 1). MRI showed masses within the internal auditory canal (IAC) ipsilateral to the periorbital hemangioma with variable extension into the cerebellopontine angle (CPA) in 3 cases, with the mass being confined to the IAC in the fourth case (Figs 1–4). Two patients demonstrated extension of the enhancing mass beyond the IAC/CPA. In one patient the mass extended along the V2 nerve into the Meckel cave and the ipsilateral cavernous sinus (Fig 2). Another patient demonstrated posterior extension of the mass into the fourth ventricle (Fig 4).

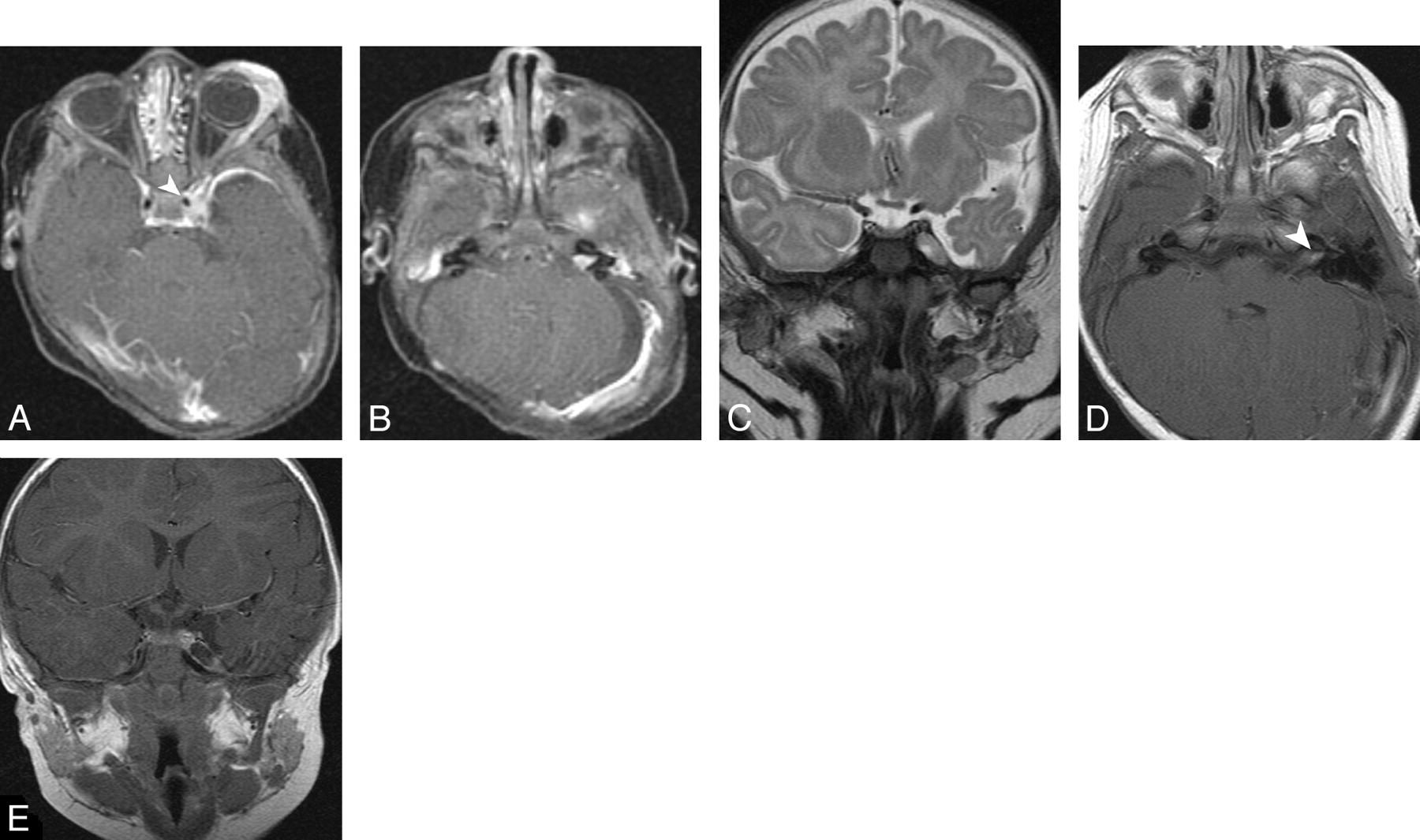
Six-week-old girl with right periorbital and IAC/CPA hemangiomas.
A, Axial T1 postcontrast image with fat suppression at presentation showing enhancing right orbital and IAC/CPA masses, relative hypoplasia of the right internal carotid artery (arrowhead), and subtle right cerebellar hypoplasia.
B, Coronal T1 postcontrast image with fat suppression at the time of presentation demonstrating the enhancing right CPA mass with a small number of flow voids.
C, D, Axial and coronal T1 postcontrast, fat-suppressed images obtained 2 months following steroid therapy with significant involution of the right IAC/CPA mass (arrowhead, D).

Eight-week-old girl with large left periorbital hemangioma extending into left cavernous sinus, Meckel cave, and the left IAC.
A, B, Axial T1 postcontrast, fat-suppressed images at presentation showing a left orbital mass and fullness of the left cavernous sinus (A), as well as a cone-shaped enhancing mass in the left IAC (B). Also evident are left cerebellar hypoplasia and relative left internal carotid hypoplasia (arrowhead, A).
C, Coronal T2 image at presentation with isointense soft-tissue mass enlarging Meckel cave on the left.
D, Axial T1 postcontrast image at 1 year follow-up showing nearly complete involution of the left IAC mass.
E, Coronal T1 postcontrast image in the same plane as panel C at 1-year follow-up showing an enlarged Meckel cave and resolution of the soft tissue mass.
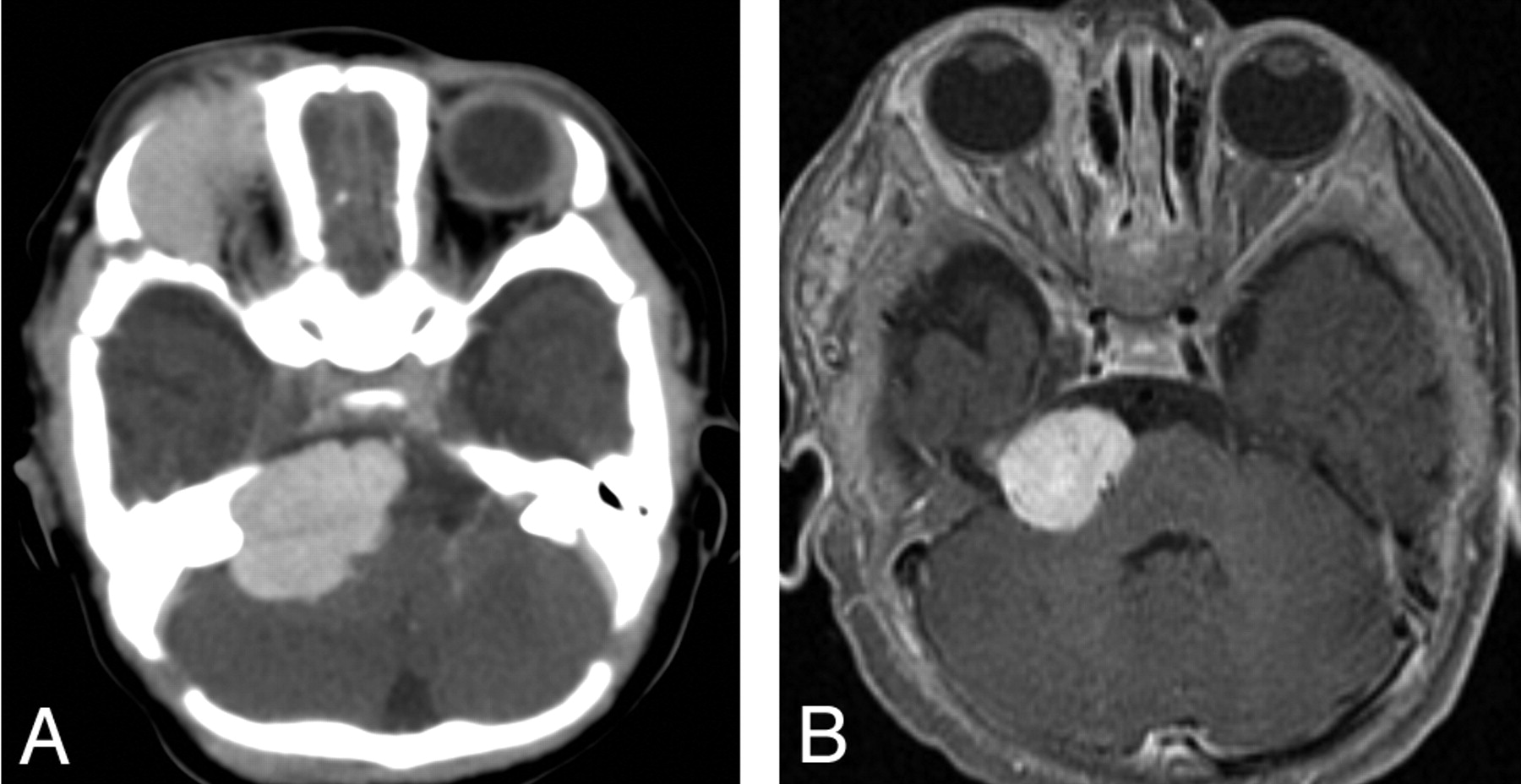
The masses were subjectively isointense to the periorbital lesion on both T1 and T2 sequences and demonstrated intense enhancement following the administration of gadolinium, closely paralleling that of the periorbital hemangiomas. Additionally, all 3 lesions contained small flow voids, resembling those seen in the periorbital lesions. The fourth patient was initially evaluated with contrast-enhanced CT and demonstrated a right periorbital hemangioma and an ipsilateral IAC/CPA mass with similar intense, venous-phase contrast enhancement (Fig 3). Some bony remodeling and widening of the IAC was also observed.

Three-week-old girl with large right periorbital and IAC/CPA hemangiomas.
A, Axial postcontrast CT at presentation showing right orbital enhancing mass with large, isoattenuated enhancing mass in the ipsilateral IAC/CPA.
B, Axial T1 postcontrast image with fat suppression at 3-month follow-up showing moderate involution of the right CPA/IAC enhancing mass. Note marked involution of right periorbital tissue.
All 4 patients underwent steroid therapy: 2 received intralesional injection of triamcinolone, and 2 received oral prednisolone. This difference in treatment likely reflects an institutional preference and trend toward intralesional therapy at the time of the later cases. Following steroid therapy, all 4 patients underwent MRI evaluation. All of the periorbital hemangiomas and intracranial enhancing masses demonstrated clear and significant involution. The 2 smaller intracranial masses showed nearly complete involution (Figs 2, 4) while the 2 larger masses demonstrated at least 30% loss of volume (Figs 1, 3).

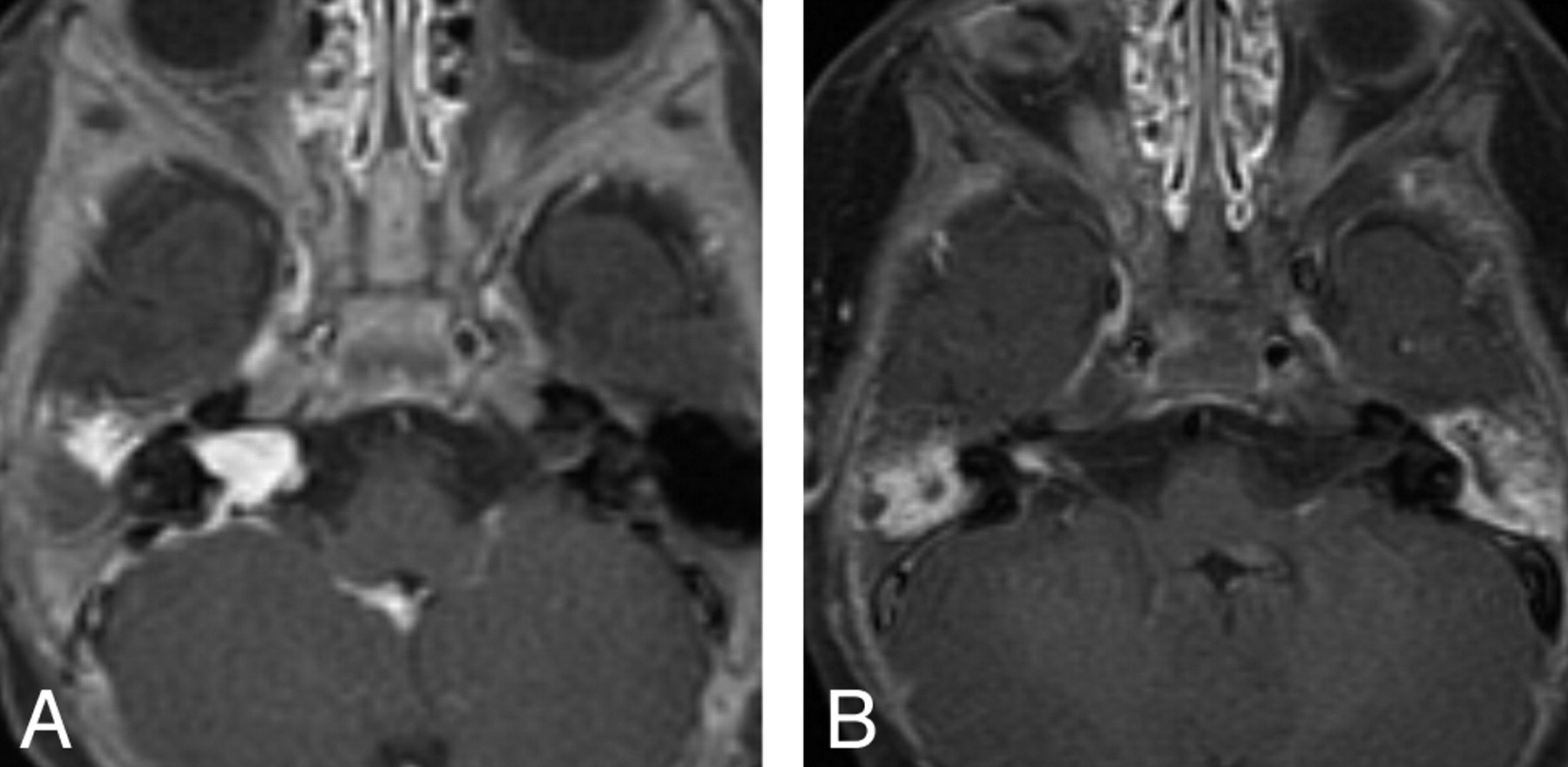
Three-week-old girl with multiple superficial hemangiomas involving the right scalp, orbit, and pinna, as well as a large right IAC/CPA hemangioma and small fourth ventricle hemangioma.
A, Axial T1 postcontrast image with fat suppression at presentation showing right IAC/CPA enhancing mass. Note ipsilateral internal carotid hypoplasia and linear enhancement in fourth ventricle.
B, Axial T1 postcontrast image with fat suppression 3 months following steroid therapy showing significant involution of the IAC/CPA mass.
Additional craniocervical abnormalities associated with PHACE syndrome were observed in all patients. All 4 patients demonstrated internal carotid hypoplasia ipsilateral to the orbital hemangioma and intracranial mass (Figs 1A, 2A, 3A). Two patients also demonstrated ipsilateral cerebellar hemispheric hypoplasia (Fig 2B). Eye abnormalities were present in 2 cases, including contralateral congenital glaucoma in one and ipsilateral persistent hyperplastic primary vitreous in another. Additional craniocervical infantile hemangiomas were present in 3 patients, involving the nasofrontal and maxillary regions in one patient, the mandibular region in another patient, and the parapharyngeal and buccal spaces in the third. None of the patients demonstrated clinical findings to suggest cardiac, aortic, or sternal defects, and thoracic imaging was not performed. No other congenital intracranial vascular anomalies or evidence of progressive intracranial arterial occlusive disease was observed.
The patient with the mandibular region hemangioma initially presented with right facial paralysis ipsilateral to the orbital hemangioma and intracranial mass. This resolved following steroid therapy. However, at 4 months of age, 9 weeks after her follow-up evaluation demonstrating involution of the periorbital and presumed intracranial hemangiomas, the patient developed stridor and was found to have a right subglottic hemangioma on bronchoscopy. Additional imaging at this time showed the intracranial and orbital lesions to be stable. The patient underwent additional oral steroid therapy with resolution of airway symptoms. At 2 years of age the patient developed enlargement of the right facial and right orbital hemangiomas and was satisfactorily treated with oral steroids and subcutaneous interferon therapy. By 4 years of age, the patient had no clinical evidence of residual or recurrent disease.
One other patient had a recurrence of the orbital hemangioma at 1 year of age that required repeat intralesional steroid therapy. The intracranial mass, however, remained stable. The 4 patients were followed variably from 1 to 4 years of age (1, 2, 2, and 4 years) with no other recurrences of the cutaneous hemangiomas observed during this time. Symptomatic follow-up imaging was recommended.
Discussion
Infantile hemangiomas, previously referred to as capillary hemangiomas, are the most common benign tumors of infancy, affecting up to 10% of children under 1 year of age.9 These lesions are true vascular neoplasms arising from unrepressed proliferation of the capillary endothelial cell. Hemangiomas are more common in white children and, as in our 4 cases, affect girls 3–5 times more often than boys. These lesions typically develop in the neonatal period but may occasionally be present at birth. Such lesions typically undergo a “proliferative” phase of rapid growth and enlargement followed by a more gradual “involuting” phase, which may take years.10 Infantile hemangiomas should not be confused with congenital vascular malformations that are present at birth, grow commensurate with the child, and do not spontaneously involute. Vascular malformations can be divided based on the predominant vessel type within the lesion as lymphatic, venous, mixed venolymphatic, arteriovenous, or capillary malformations.9
The association of cervicofacial infantile hemangiomas with vascular anomalies and intracranial malformations was first recognized by Pascual-Castroviejo in 1978.3 Pascual-Castroviejo subsequently termed the disorder cutaneous hemangioma–vascular complex syndrome. Although this term is still used, particularly in the European literature, the name PHACE syndrome has gained popularity recently. In 1996 Frieden et al coined the acronym PHACE for the neurocutaneous syndrome linking posterior fossa malformations (P), cervico-facial hemangiomas (H), arterial anomalies (A), cardiac defects/aortic coarctation (C), and various eye abnormalities (E).8 Some authors also include sternal defects and refer to the syndrome as PHACES syndrome.4 Most previous studies have stressed the heterogeneity of the syndrome, and strict criteria of inclusion or exclusion have not been universally developed. The common denominator in the syndrome is the facial hemangioma, typically described as plaquelike and segmental in appearance.10 Although some authors think that the distribution of the hemangiomas are random, recent studies have strongly suggested a dermatomal distribution.8,10,11
The underlying pathogenesis of PHACE syndrome remains speculative. Although involvement of the neural crest has been implicated, a single defect responsible for all the manifestations has not been found. There is a strong female predominance, leading some to suggest an X-chromosome-linked dominant condition, potentially lethal in males. However, no familial tendency has been reported. Several lines of evidence have suggested an insult occurring between 5 and 10 weeks’ gestational age, resulting from errors affecting regulatory genes that determine morphogenesis of several tissue types.8,10
The intracranial findings associated with PHACE syndrome include developmental anomalies of the posterior fossa and various abnormalities of the intracranial arteries. Posterior fossa abnormalities range from the classic Dandy-Walker malformation to cerebellar hypoplasia and arachnoid cysts. The arterial anomalies include internal carotid artery hypoplasia, persistent fetal arteries, and progressive internal carotid artery occlusion that mimics Moyamoya disease.10,12 Interestingly, all 4 cases presented here demonstrated varying degrees of ipsilateral internal carotid hypoplasia, and patients 1 and 2 demonstrated ipsilateral cerebellar hypoplasia.
Because of their rarity, the recognition of associated intracranial hemangiomas has occurred relatively recently. In the original report in 1978, Pascual-Castroviejo described a single case of intracranial “angiomatous malformations” in a patient with facial hemangioma.3 In 1996, Frieden et al described a 2-cm enhancing CPA lesion, consisting of “abnormal blood vessels,” in a patient with ipsilateral facial hemangioma. 8 In 1999, Tortori-Donati et al described 4 infants with a variety of imaging findings associated with facial hemangiomas.2 In particular, all 4 patients had “intracranial contrast-enhancing masses.” Based on the general radiologic features of the intracranial lesions, their radiologic similarity to the cutaneous hemangiomas, and the fact that 2 of the intracranial lesions underwent partial involution during follow-up, the authors suggested the diagnosis of intracranial “capillary” hemangioma, an otherwise rare lesion. No biopsies were performed.
Since then, intracranial infantile hemangiomas have been the subject of sporadic case reports, mostly in association with PHACE syndrome. In 2002, Poetke et al reviewed the literature and reported 10 new cases of PHACE syndrome, including a single patient with several intracranial enhancing lesions.5 These authors again suggested the diagnosis of intracranial hemangiomas and further proposed that this finding be included as a separate diagnostic criterion for the PHACE syndrome, given that intracranial infantile hemangiomas are rarely found in isolation. In their review of the literature they also noted that the incidence of intracranial hemangiomas in patients with PHACE syndrome (12%) is greater than that of coarctation of the aorta (10%), subglottic hemangiomas (7%), or ventral developmental defects (5%). Bhattacharya et al then presented 8 new cases of PHACE syndrome in 2004, including a single patient with concomitant orbital and ipsilateral CPA hemangiomas.4 In 2005, Ersoy and Mancini reported a single case of an intracranial hemangioma in a patient with a large facial and scalp hemangioma.1 Given that the patient had no other findings, these authors suggested that the association of intracranial hemangiomas and facial hemangiomas might occur in the absence of PHACE syndrome.
Any discussion of PHACE syndrome is inherently difficult. Even the name of the syndrome is not universally accepted. The rarity of the syndrome, the lack of a unifying pathophysiologic mechanism, and the marked variety of clinical and imaging manifestations all lead to potential controversy. Additionally, the absence of pathologic evaluation of any reported intracranial lesion leaves room for debate about their true nature. The cases presented here are similar to those previously described in the literature as part of PHACE syndrome. The inclusion of these 4 cases is supported by the associated findings of cerebellar hypoplasia, carotid hypoplasia, and the presence of other extracranial hemangiomas.
We submit that these additional 4 cases support the diagnosis of intracranial infantile hemangiomas, despite the lack of surgical excision or biopsy. These lesions are typically dural based and have a predilection for the ipsilateral skull base. The most consistent location was the ipsilateral IAC with variable extension into the CPA. Lesions were also noted in the cavernous sinus, the Meckel cave, and the fourth ventricle. All lesions demonstrated marked contrast enhancement, and flow voids were visible in some. All lesions were strikingly similar to the clinically obvious periorbital hemangiomas and demonstrated at least some degree of involution following steroid therapy, with biologic response grossly paralleling that of the periorbital lesion.
Only one patient had a cranial nerve deficit (patient 3, facial palsy), potentially caused by the IAC lesion. Interestingly, no other reported cases were associated with facial nerve palsy, deafness, or vestibular signs. Of note, none of our patients had significant cardiac findings and there was no indication of aortic coarctation. This finding is in agreement with those of other authors.1-7
Conclusion
We think that these 4 cases make a significant contribution to the growing recognition of a relatively unique radiographic association that is likely related to, if not a subset of, the PHACE syndrome. Infantile hemangiomas should be considered in the differential for extra-axial enhancing lesions in infants, particularly if they are located in the IAC/CPA and associated with other features of PHACE syndrome.
Footnotes
Paper presented at: Annual Meeting of the American Society of Head and Neck Radiology, September 2005; San Francisco, Calif.
References
- Received December 23, 2005.
- Accepted after revision March 1, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Neuroaxial Infantile Hemangiomas: Imaging Manifestations and Association with Hemangioma Syndromes
- Asymmetric Meckel Cave Enlargement: A Potential Marker of PHACES Syndrome
- Enlargement of the Internal Auditory Canal and Associated Posterior Fossa Anomalies in PHACES Association
- Cervical and Intracranial Arterial Anomalies in 70 Patients with PHACE Syndrome