
Abstract
SUMMARY: Amyloidosis is a term applied to a diverse group of disorders that share the deposition of amyloid protein in various extracellular tissues. Systemic amyloidosis may involve almost any organ system in the body including regions in the head and neck; however, pharyngeal involvement is rare, with only 12 cases having been previously reported. Ten of these cases were localized disease, and only 2 cases were systemic amyloidosis. We present the case of a patient with severe diffuse systemic amyloidosis with extensive involvement of the pharynx, larynx, trachea, lungs, eyelids, and breasts. We also review the imaging characteristics and pertinent literature.
Amyloidosis is a rare, infiltrative condition characterized by deposition of abnormal protein in various tissues. When systemic amyloidosis involves regions of the head and neck, the larynx and trachea are the most common sites. To date, there have been only 2 prior reported cases of systemic amyloidosis involving the pharynx. We present a case of severe diffuse systemic amyloidosis in the chest, head and neck, with extensive involvement of the pharynx and we review the literature.
Case Report
The patient was a 64-year-old woman with a history of myasthenia gravis for 30 years, type 1 diabetes mellitus, and amyloidosis for 4 years. In the past, the patient was found to have amyloid deposits in the eyelids and breasts. A biopsy confirmed findings consistent with the AL type (amyloid light chain) of amyloidosis. The patient presented with increased shortness of breath and hoarseness on the most recent hospital admission. There was no past medical history of renal failure or multiple myeloma. The patient was being treated for myasthenia gravis with pyridostigmine (Mestinon) and high-dose steroids and had received plasmapheresis therapy in the past. Physical examination was significant for bilateral ptoses and indurations of the eyelids, pharyngeal fullness, shortness of breath, and a decreased range of motion of the neck. Her urine was negative for Bence-Jones protein, and the results of serum protein and urine protein electrophoreses were unremarkable.
A tracheostomy was performed, and a high-resolution chest CT study showed extensive interstitial lung disease, abnormally attenuated breast tissue (Fig 1) for the patient's stated age, and small nodules in the tracheal mucosa with marked thickening of the tracheal wall with significant stenosis (not shown). An endoscopic examination of the trachea revealed nodular deposits and plaques on the mucosal surface along its entire length. Noncontrast MR imaging of the neck was performed on a 1.5T magnet. Contrast was not administered because of a reported allergy to gadolinium. The images showed large submucosal, nodular masses in the pharynx and supraglottic larynx, and thickening of the tracheal wall with stenosis. These masses had intermediate T1-weighted signal intensity (Figs 2A) and low T2-weighted signal intensity (Figs 2B, C, D). The large submucosal supraglottic laryngeal deposits were the primary cause of her airway obstruction. These findings on imaging were consistent with systemic amyloidosis. Biopsy specimens of the tracheal wall deposits on the mucosal surface confirmed the diagnosis of AL-type amyloidosis.

Axial noncontrast CT of the chest shows abnormally attenuated nodular breast tissue bilaterally and focal nodularity (arrows) along the right posterior pleura.

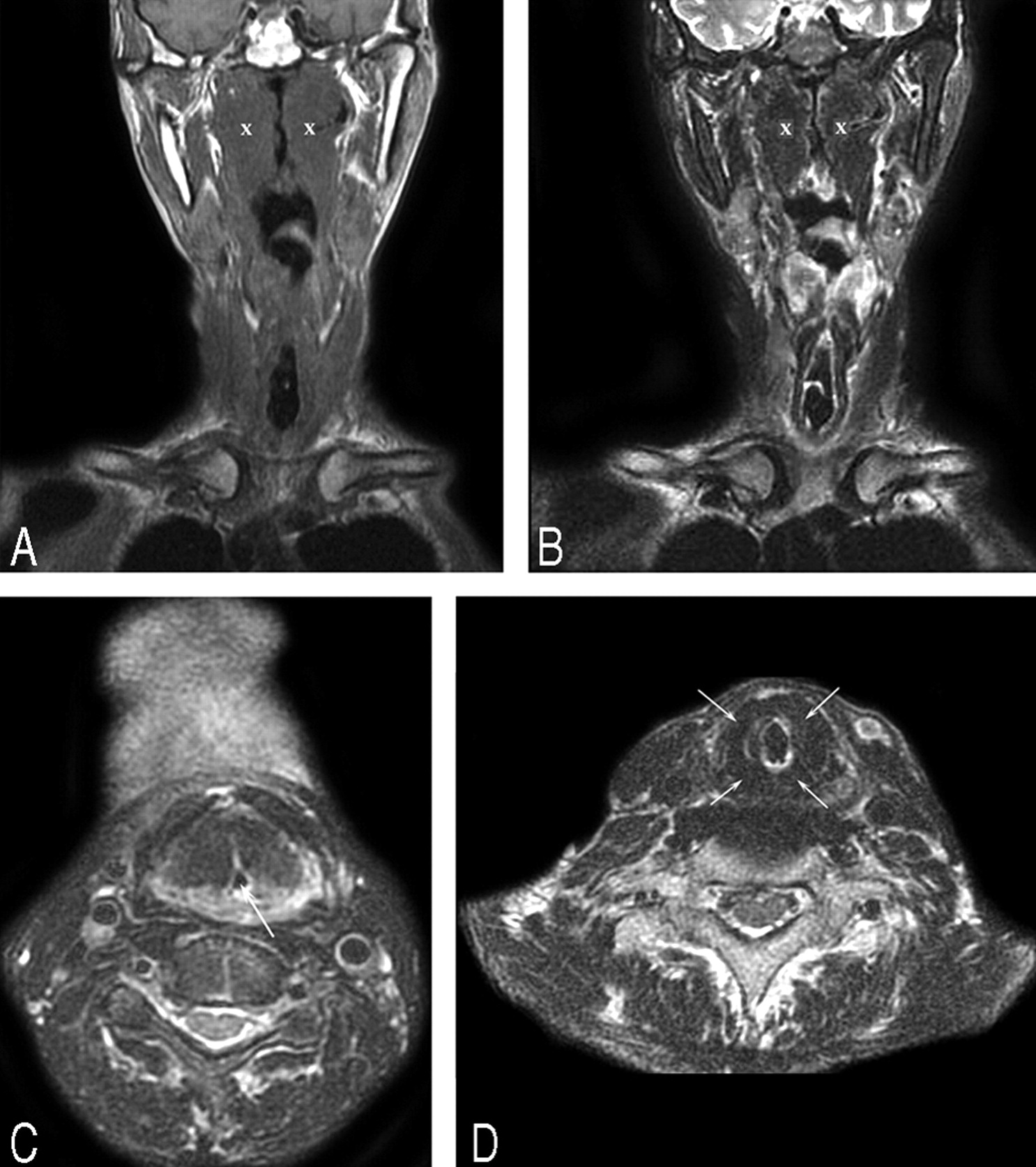
Noncontrast MR images show large nodular, submucosal masses along the pharyngeal walls, supraglottic larynx, and thickening of the tracheal wall with stenosis. Note the extensive involvement of the nasopharynx and oropharynx. A, Coronal T1-weighted MR image shows the pharyngeal masses (x) to have intermediate signal intensity. B, Coronal T2-weighted MR image shows the masses (x) to have low signal intensity. The signal intensities of the masses parallel those of skeletal muscle. C, Axial T2-weighted MR image shows the masses to have low signal intensity. There is marked narrowing of the laryngeal airway (arrow). D, Axial T2-weighted MR image shows marked low signal intensity thickening (arrows) of the tracheal walls.
Discussion
Amyloidosis is a condition characterized by infiltration and extracellular deposition of homogeneous, eosinophilic proteinaceous fibrils in a beta-pleated sheet configuration. It classically has an apple-green birefringence when stained with Congo red and viewed under polarized light. From a clinical standpoint, it may be classified as a localized or systemic disease. The localized disease involves only 1 organ, typically the larynx or brain (where it has been associated with aging and Alzheimer disease). Systemic amyloidosis involves many organ systems and is typically divided into 3 separate categories. Primary amyloidosis (AL type or amyloid light chain) is the result of spontaneous overproduction of the antibody light chain in the bone marrow plasma cell. Secondary amyloidosis (AA type or amyloid A protein) occurs as a result of an underlying condition such as multiple myeloma; chronic infections (tuberculosis or osteomyelitis); and chronic inflammatory diseases such as rheumatoid arthritis, Sjögren disease, and ankylosing spondylitis. The familial type (ATTR type, or amyloid transthyretin protein) is rare and exhibits an autosomal dominant pattern of inheritance, and the amyloid deposits are composed of the protein transthyretin, which is made in the liver. There are 12 other protein subtypes that have been identified but are far less common.1–4
From a radiographic standpoint, MR imaging is the technique of choice to demonstrate the most specific features of amyloidosis. Typically, the amyloid deposits have intermediate T1-weighted signal intensity and low T2-weighted signal intensity, similar to skeletal muscle. This is secondary to the beta-pleated structure of the amyloid deposits that occurs as protein fibrils in a parallel sheetlike configuration, similar to the organization of skeletal muscle fibers. Because of these unique imaging features, MR imaging is considered to be a more specific technique than CT to establish the diagnosis of amyloidosis.1,5
In systemic primary amyloidosis, deposits in the region of the head and neck are uncommon. However, the most common head and neck sites are the supraglottic and subglottic larynx as well as the thyroid gland.4,6,7 There were 12 previous cases that date back to 1980.8 Of these 12 cases, 10 were of localized disease of the nasopharynx. In the cases of localized disease, systemic amyloidosis was ruled out by either abdominal or rectal biopsy.2–10 There were only 2 previous cases in the literature of systemic amyloidosis (both AL type) that involved the pharynx.11,12 The current case is an example of a patient with severe systemic amyloidosis with diffuse involvement of the pharynx.
Amyloidosis of the breasts is also a rare entity and has been described in only 35 cases since 1973.13 Ten of these cases were of the AL systemic type and were not associated with an underlying condition.13 In systemic amyloidosis, involvement of the eyelids can occur, but orbital involvement is uncommon.14 It is usually localized, and the imaging features are similar to those described above.14
Amyloidosis, either systemic or localized, may affect the upper and lower respiratory tract.15 In amyloidosis of the lung, the imaging characteristics are diverse and therefore may mimic a variety of pathologic processes in the lung.16 Tracheobronchial amyloidosis is characterized by amyloid deposits in the trachea and large bronchi, with extension at times into segmental bronchi.17 Tracheal stenosis often results from thickening of the tracheal wall. Any inflammatory or granulomatous process demonstrates similar features as amyloid on CT.18,19 However, on MR imaging, the signal intensities mentioned above should suggest the diagnosis.13,20
Systemic amyloidosis carries a poor prognosis because accumulation of amyloid fibrils in the tissues destroys normal structure and function. However, the localized form of amyloidosis carries a much better prognosis. Therefore, it is important to identify the presence of amyloid on imaging by using the characteristics described and then determine whether this is localized or systemic disease.
Conclusion
Amyloidosis is a rare, infiltrative condition characterized by deposition of abnormal protein in various tissues. When systemic amyloidosis involves regions of the head and neck, the larynx and trachea are the most common sites. To date, there have been only 2 previous reported cases of systemic amyloidosis involving the pharynx. We described the case of a patient with severe systemic amyloidosis who presented with airway obstruction as a result of extensive involvement of the larynx, trachea, nasopharynx, and oropharynx. We also reported the findings on imaging. There was also a review of the literature of amyloid deposits in the pharynx.
References
- Received November 30, 2006.
- Accepted after revision January 20, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}