
Abstract
BACKGROUND AND PURPOSE: The safety and efficacy of the Woven EndoBridge (WEB) device has been shown in multiple good clinical practice trials, whereas aneurysm locations in these trials were restricted to bifurcation aneurysms located at the circle of Willis (MCA bifurcation, ICA bifurcation, anterior communicating artery, basilar artery tip). Our aim was to evaluate angiographic and clinical results with the WEB 17 in aneurysm locations that were excluded from the good clinical practice trials, assuming that the angiographic and clinical results are similar to those of the good clinical practice trials for aneurysms in traditional locations.
MATERIALS AND METHODS: We performed retrospective analysis of immediate and follow-up results of aneurysms in locations outside the good clinical practice trials in which the WEB 17 was used on an intention-to-treat approach.
RESULTS: Between June 2017 and May 2020, forty-seven aneurysms in 44 patients met the inclusion criteria. Aneurysm locations were the ICA posterior communicating artery in 19 (40.3%), the ICA paraophthalmic or choroidal locations in 4 (8.6%), anterior cerebral artery A2 segment in 13 (27.7%), MCA M1 segment in 2 (4.3%), posterior cerebral artery P2 segment in 2 (4.3%), PICA in 3 (6.4%), and the superior cerebellar artery in 4 (8.4%) cases. The procedure-related morbidity and mortality rates in the entire series were 0.0%. The early and late (<12 and >12 months) complete occlusion rates were 63.9% (23/36) and 77.8% (14/18), respectively.
CONCLUSIONS: The WEB 17 is safe and effective in aneurysm locations different from the traditional bifurcation aneurysms included in the good clinical practice trials. Further studies will help to define the entire spectrum of aneurysm morphologies and locations suitable for the WEB 17.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- bif
- bifurcation
- BOSS
- Bicêtre Occlusion Scale Score
- GCP
- good clinical practice
- PcomA
- posterior communicating artery
- RROC
- Raymond-Roy Occlusion Classification
Intrasaccular flow disruption has emerged as an effective and safe endovascular treatment option for complex intracranial aneurysms that may be otherwise difficult to treat. Positive results from numerous retrospective and prospective studies involving the Woven EndoBridge (WEB; MicroVention) have contributed to the growing popularity of the WEB for intrasaccular flow disruption. The WEB device was initially intended for the treatment of broad-based bifurcation aneurysms because these aneurysms are difficult to treat without additional neck-bridging devices or stents. Therefore, in most studies using the WEB, bifurcation aneurysms were analyzed.1⇓⇓⇓-5 Experience with the WEB is increasing with a rapidly growing number of cases since its introduction in 2011, while the device simultaneously underwent several revisions and innovations with the addition of smaller sizes of both the device and the delivery microcatheter. The visibility of the device was enhanced, and the number of wires making up the device was reduced without affecting of the hemodynamic efficacy. While the first-generation systems required comparatively large and difficult-to-navigate microcatheters for delivery (0.033 and 0.027 inch), the latest systems are compatible with 0.017-inch microcatheters. Recent studies regarding the WEB 17 supported an expansion of indications toward smaller and more distal aneurysms.6⇓⇓-9 In addition, the use of the WEB in aneurysm locations distinct from the traditional bifurcation locations is becoming more recognized in clinical practice.
In this retrospective study, we sought to evaluate the angiographic and clinical results in the endovascular treatment of aneurysms in locations that were excluded from previous studies with the WEB device. We hypothesized that the angiographic and clinical results in this specific subgroup of aneurysms are comparable with those of traditional bifurcation-type aneurysms, possibly widening the applications for intrasaccular flow disruption.
MATERIALS AND METHODS
Study Design and Data Analysis
We retrospectively reviewed the institutional data bases of 2 neuroendovascular centers regarding the endovascular treatment of ruptured and unruptured intracranial aneurysms treated with the WEB 17 device between June 2017 and May 2020. Aneurysm locations that met the inclusion criteria of good clinical practice (GCP) studies of the WEB device were excluded.1⇓-3,10 The excluded locations were the MCA bifurcation (bif), the anterior communicating artery, the ICA bif, and the tip of the basilar artery. The remaining aneurysm locations treated with the WEB 17 system were the following: the ICA at the paraophthalmic segment, the posterior communicating artery (PcomA) or the origin of the anterior choroidal artery (ICA choroid), the MCA M1, the A2 segment of the anterior cerebral artery (ACA A2), the P2 segment of the posterior cerebral artery (P2), the PICA, and the superior cerebellar artery. The aneurysms meeting the location criteria were included in further analysis according to the study design presented by Pierot et al,11 who, with this approach, analyzed predecessor versions of the WEB device in 2017. Minor subsets of our study population were previously included in an overall analysis of the WEB 17 system.8
The decision for endovascular treatment of unruptured aneurysms was reached by consensus in a weekly interdisciplinary board meeting at each participating center, while the final treatment strategy was determined by the operator. In patients with rupture, the treatment decision was made by the responsible neuroradiologist and neurosurgeon. Only cases in which the WEB 17 was considered on an intention-to-treat approach without adjunctive devices were included. Because this was a retrospective observational analysis, inclusion or exclusion criteria were not prospectively defined. A dome-to-neck ratio of <2 indicated a broad-based anatomy as an indication for treatment, but morphologies with a defined neck were not excluded if the configuration of the aneurysm appeared suitable for treatment with the WEB device. Alternative treatment strategies included standard coiling, remodeling, stent-assisted coiling, or flow diversion. Treatment with the WEB is increasingly considered as a first-line approach in broad-based aneurysms whenever possible to avoid long-term dual-antiplatelet therapy as needed for stent-assisted coiling or flow diversion. Absolute criteria against treatment with the WEB 17 were an aneurysm morphology or size unsuitable for the given range of WEB 17 devices (maximum diameter, <2.0 or >6.5 mm) according to the manufacturer’s sizing guide, an incorporation of branches into the aneurysmal sac, or a neck diameter larger than the maximum fundus diameter.7,8
We included the following clinical and angiographic data: demographic patient data; clinical status on admission, at discharge, and at each follow-up visit measured by the mRS; aneurysm location; rupture status; fundus and neck size; dome-to-neck ratio; type and size of the WEB 17 device deployed; technical success (navigation and deployment of the WEB); rate of unplanned additional devices applied for “bail out” adjunctive treatments (eg, stents, coils); occlusion rates at each follow-up visit (scheduled 3–6 and 12 months after treatment); and complications.
Occlusion rates were initially evaluated according to the Bicêtre Occlusion Scale Score (BOSS), which is scaled as follows: 0 = no residual flow inside the aneurysm or the WEB; 0′ = opacification of the proximal recess of WEB; 1 = residual flow inside the WEB; 2 = neck remnant; 3 = aneurysm remnant; and 1 + 3 = contrast media depicted inside and around the device.12 In the final descriptive analysis, these results were “translated” to the 3-point Raymond-Roy Occlusion Classification (RROC). BOSS grades 0 and 0′ were classified as complete occlusion (RROC grade I), whereas BOSS grades 1 and 2 were recorded as neck remnants (RROC grade II). Correspondingly, BOSS grades 3 and 1 + 3 describe an aneurysm remnant (RROC grade III).11⇓-13
Angiographic results were independently analyzed and classified in a blinded fashion by 2 experienced neurointerventionalists. In cases of inconsistency concerning the final result, a decision was made by consensus.
Procedure-related complications that resulted in a clinical sequelae of at least 1 point on the mRS scale defined the procedure-related morbidity and mortality.
WEB Treatment
The technical specifications of the WEB 17 device were previously described.7,8 Sizing of the WEB 17 device resulted from calibrated measurements of the aneurysm height and width in 2 orthogonal projections assisted by the manufacturer’s sizing calculator based on the principle of slightly oversizing the device width with compensatory undersizing of its height.7,8
Procedures were exclusively performed on a biplane angiographic system with the patient under general anesthesia via transfemoral access. All devices were implanted using a VIA 17 microcatheter (MicroVention). In elective cases, patients were placed on a dual-antiplatelet therapy in preparation for the procedure according to the standards at the 2 centers. Ruptured aneurysms were treated without dual-antiplatelet therapy. All procedures were performed with 5000 IU of heparin given intravenously at the beginning of the procedure.
Statistical Analysis
The statistical analysis of all variables was performed independently using Excel (Microsoft). Continuous variables are given as the median and range, and independent variables are described as percentages.
Ethics Statement
The study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study received approval from the local ethics committee. A separate informed consent from each patient before inclusion in this retrospective study was not required according to the guidelines of the responsible ethics committee.
RESULTS
Patient and Aneurysm Population
Between June 2017 and May 2020, a total of 198 intracranial aneurysms were treated with the WEB 17 device. Of those, 47 aneurysms in 44 patients (median age, 55 years; range, 39–78 years; 32 women) met the defined inclusion criteria of aneurysm locations treated with the WEB 17 device. Of the 47 aneurysms, 32 (68.1%) were found incidentally, 13 (27.7%) were treated in the acute (within 48 hours) phase of SAH from the target aneurysm, and 2 (4.3%) were remnants of previously coiled aneurysms. Thirty-eight (80.9%) aneurysms were located in the anterior circulation, and 9/47 (19.1%) were posterior circulation aneurysms. The median aneurysm fundus diameter was 3.0 mm (range, 2.0–6.5 mm), and the median neck width was 2.0 mm (range, 2.0–6.0 mm). Most aneurysms (41/47, 87.2%) had a dome-to-neck ratio of <2.
Table 1 summarizes the locations and morphologic features of the treated aneurysms.
Angiographic characteristics of the WEB 17-treated aneurysms
Procedural Details and Complications
Treatment was successfully performed with the WEB 17 in all cases, meaning that a switch to an alternative treatment strategy due to a failed attempt to implant the WEB 17 did not occur. In 1 case, coils were used in addition to the WEB as part of the treatment strategy. This was an incidental ICA PcomA aneurysm with an upper lobule that was occluded with coils using a previously placed microcatheter after implantation of a WEB (WEB Single-Layer [SL] 7 × 3) into the aneurysm fundus.
The overall rate of complications in the entire series was 6.4% (3/47) to date. In 2 cases, a Neuroform Atlas Stent (Stryker) was placed as a bailout treatment to stabilize the WEB device and preserve the parent artery. One was a ruptured ICA choroidal aneurysm that was catheterized with the VIA 17 microcatheter, and a WEB device (WEB SL 5 × 3) was positioned within the aneurysm without problems, even though the angle between the longitudinal axis of the aneurysm and the parent artery was comparatively high (about 90°). Once the device was detached, it partly dislocated into the ICA. The operator performed a mild percutaneous transarterial angioplasty with a compliant balloon followed by implantation of a Neuroform Atlas stent to secure the WEB device and preserve the ICA. The postinterventional CT did not show any ischemic lesions, and the patient was discharged with an mRS score of 1 that was most likely related to the SAH.
In the second case, a ruptured ACA A2 aneurysm was treated with a WEB (WEB SL 3.5 × 2) with the base of the device slightly protruding into the parent artery. There was no evidence of flow disturbance or formation of thrombus; however, the operator decided to deploy the Neuroform Atlas stent to stabilize the WEB device. The third complication was a ruptured ACA A2 aneurysm treated with a WEB (WEB SL 3.5 × 2) initially without problems. Following detachment of the device, the angiographic run showed a thrombotic occlusion of a small branch originating in close vicinity of the aneurysm. The occlusion resolved within 30 minutes after 500 mg of acetylsalicylic acid was given intravenously and the systolic blood pressure was moderately elevated.
All 3 patients remained without clinical sequelae, resulting in procedure-related morbidity and mortality of 0.0% in the entire series. Of the 13 patients who presented with an SAH from the target aneurysm, one died during hospitalization.
Immediate and Follow-up Angiographic Results
Of the 47 aneurysms treated, 15 (31.9%) showed an immediate complete occlusion (RROC I) directly after implantation of the WEB 17 device, while the remaining 32 aneurysms (68.1%) showed a beginning stagnation of contrast media within the aneurysm (RROC II and III).
To date, a single follow-up angiography performed within the first 12 months after treatment is available for 36 aneurysms in 34 patients, obtained after a median of 4 months (range, 1–10 months). Of those, 23/36 (63.9%) aneurysms showed complete occlusion (RROC I) and 13/36 (36.1%) had a neck remnant (RROC II). Of the 13 aneurysms with a neck remnant, 9 were ICA PcomA aneurysms, while the median fundus size was 4.0 mm (range, 2.0 −6.5 mm). There were 2 cases in which a “crushing” of the WEB was observed.
A second follow-up angiography performed after the first 12 months was completed for 18 aneurysms in 17 patients after a median of 15.5 months (range, 12–24 months). The rate of complete occlusion (RROC I) was 77.8% (14/18 aneurysms) with 22.2% (4/18) showing a neck remnant (RROC II).
A summary of the follow-up results is given in Table 2.
Immediate and follow-up results of the treated aneurysms according to the BOSS classification12
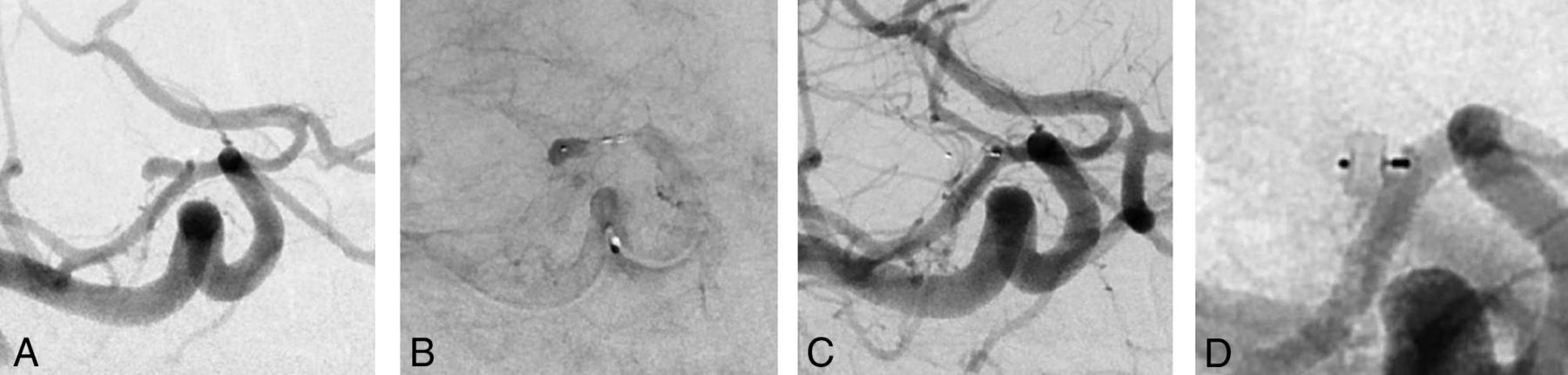
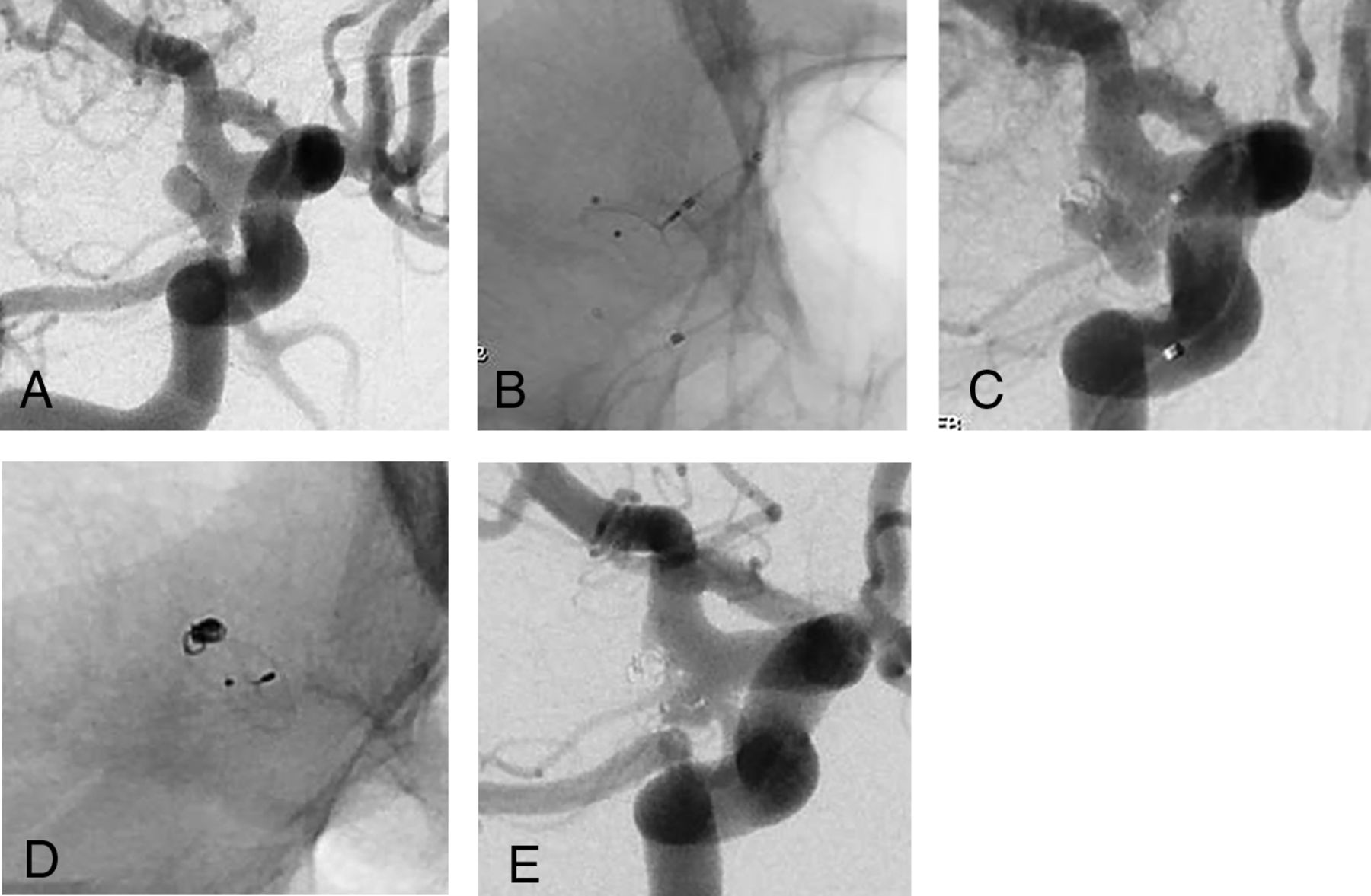
Two cases of a ruptured MCA M1 and an incidental ICA PcomA aneurysm treated with the WEB 17 device alone and in combination with coils are presented in Figs 1 and 2.

A, Acutely ruptured aneurysm of the MCA M1 segment in a 40-year-old female patient, right anterior oblique view, cranial angulation. B, Stasis of contrast media within the aneurysm after placement of a 3.5 × 2 mm WEB SL device, right anterior oblique view, cranial angulation. C, Prompt occlusion of the aneurysm after detachment of the WEB device, right anterior oblique view, cranial angulation. D, Twelve-month follow-up angiography reveals a stable and complete occlusion of the MCA M1 aneurysm.

A, Incidental finding of a “bean-shaped” ICA PcomA aneurysm in a 44-year-old male patient, right anterior oblique view, caudal angulation. B, Placement of an Excelsior SL 10 microcatheter (Stryker) inside the upper lobe of the aneurysm followed by a WEB SL 7 × 3 placed within the aneurysm fundus, fluoroscopy, right anterior oblique view, caudal angulation. C, Coil occlusion of the upper lobe of the aneurysm not completely covered by the WEB device, right anterior oblique view, caudal angulation. D, Three-month follow-up angiography demonstrates a crushing of the WEB device, fluoroscopy, right anterior oblique view, caudal angulation. E, Evidence of a neck remnant due to the crushing of the WEB device on the 3-month follow-up angiography, right anterior oblique view, caudal angulation.
DISCUSSION
Intrasaccular flow disruption is currently a well-established treatment option for broad-based intracranial aneurysms. The effectiveness of the WEB device as the most widely used flow disruptor was demonstrated in several prospective GCP studies. The inclusion criteria of the WEBCAST, WEBCAST 2, French Observatory, and WEB-IT studies for aneurysm location were restricted to bifurcation aneurysms of the MCA, anterior communicating artery, ICA bif, and basilar artery tip, and most aneurysms treated in those studies were broad-based. The complete aneurysm occlusion rate of aneurysms treated with WEB at 1 year in the WEBCAST, WEBCAST 2, and French Observatory studies was 52.9%, with similar results reported for the WEB-IT study (58.3%).1⇓-3 Following these results, the WEB device received FDA approval for broad-based, saccular aneurysms in the aforementioned locations.
The introduction of the WEB 17 system, not yet available for the mentioned studies, was a further step toward a lower device profile with an enhanced controllability, mainly due to the compatibility with a 0.017-inch microcatheter. Initial results with the WEB 17 device support an expansion of indications toward more distally located, smaller aneurysms.7,8 This trend is evident in the inclusion criteria of an ongoing GCP study on the WEB 17 device, with no defined location excluded in contrast to the previous GCP studies.14
We sought to evaluate the safety and efficacy of the WEB 17 system in the specific subgroup of aneurysm locations that were excluded from prior GCP studies. Our hypothesis was that the angiographic success and safety profile would be comparable with those of bifurcation-type aneurysms in the “traditional” locations. Our short- and long-term complete occlusion rates of 63.9% and 77.8% with a procedure-related morbidity and mortality of 0.0% are in line with the results of prior GCP studies.
The restriction to bifurcation aneurysms in the initial GCP trials conducted with the predecessor versions of the WEB device is mainly explained by the smaller angle between the parent artery and the aneurysm in bifurcation anatomies compared with sidewall aneurysms, where the angle is usually higher. Correct positioning of the WEB device with good apposition to the aneurysmal wall, including an exact reconstruction of the neck area, results from a controlled forward pushing of the partially unfolded device.15 This maneuver as well as the initial catheterization becomes more challenging in anatomies with a higher angle between the aneurysm and the parent artery because the forward force applied to the microcatheter is vectored along the parent artery. The possibility of using a 0.017- inch microcatheter facilitates the catheterization in highly curved anatomies. Furthermore, the deviation of the (preshaped) microcatheter induced by the application of the WEB device is lower with the WEB 17 system due to the lower profile compared with the predecessor version. Thus, the transmission of force along a higher angle might be more efficient due to the softer structure of the WEB 17 system.
To date, there are only limited data on the WEB device in aneurysm locations outside the traditional study indications, and the existing literature is restricted to the predicate versions of the WEB. Pierot et al,11 in 2017, were the first to present 20 patients with 20 aneurysms in “atypical locations” treated with the WEB device. Five of those were ruptured, and most were aneurysms of the anterior circulation (9 paraophthalmic segments of the ICA, 4 ICA PcomAs; 5 of ACA A2). The mean aneurysm width was 5.4 mm, while 50.0% were broad-based (neck diameter, ≥4.0 mm). Implantation of the WEB using VIA 0.021-, 0.027-, or 0.033-inch microcatheters was successful in all aneurysms without adjunctive devices needed. The treatment-related morbidity and mortality at discharge were 0.0%. The complete occlusion rate after the mean follow-up period of 7.4 months in 17 aneurysms was 82.4%. Most interesting, this rate is superior to the 52.2% and 58.3% complete occlusion rates achieved in aneurysms in typical locations within the above-mentioned GCP studies. Furthermore, these results are slightly superior to the rate of complete occlusion found in our series, even though a direct comparison is generally difficult due to the heterogeneity of the populations treated with different versions of the WEB device.
In another series of 20 ICA aneurysms (10 paraophthalmic segments of the ICA, 9 ICA PcomAs, 1 ICA choroid) treated with the WEB device, implantation of the WEB failed in 2 aneurysms (both paraophthalmic ICAs), likely due to the sharp angle between the aneurysm and the ICA. In 7 cases, additional devices (coils/stents) were used, while 60% of the aneurysms were wide-neck (neck diameter, ≥4.0 mm, or dome-to-neck ratio, <2), and the aneurysms were larger (mean aneurysm width, 8.1 mm) compared with our cohort, which is explained by the different versions of the WEB devices used. The procedure-related morbidity and mortality rates in this series were 0.0%, with a complete occlusion rate of 76.5% after a mean follow-up period of 9.6 months.16
The most recent series of the WEB device in off-label locations was presented by Zanaty et al,17 in 2020. Eleven patients with 12 aneurysms were treated using predecessor WEB devices without the VIA 0.017- inch microcatheter. Again, most were ICA aneurysms, and aneurysms were larger compared with those in our series (mean width, 8.0 mm; mean neck, 5.0 mm). Adjunctive devices were necessary in 3 cases (additional coiling in 2; stent in 1). They observed no procedure-related clinical sequelae, and the early complete and adequate occlusion rates were 33.3% and 66.7%, respectively.
Of the 13 cases with a neck remnant at the early follow-up angiography in our series, most (n = 9) were ICA PcomA aneurysms that were slightly larger than the aneurysms in the entire group. Besides the plausible factor of size, another possible explanation for the higher rate of ICA PcomA aneurysms might be found in the tight angle between the aneurysm and the parent artery in those aneurysms, which might impede an ideal position of the WEB with its hemodynamically active bottom vectored toward the parent artery. This theory might furthermore explain the 2 cases of crushing of the WEB device. However, these explanations remain hypothetic because factors determining recurrence or incomplete occlusion at the early follow-up examination were not analyzed in detail in our study due to the small sample size.
The aneurysms treated in our series were mainly small (fundus range, 2.0–6.5 mm; median, 3.0 mm). This feature is explained by the miniaturization of the device compared with predecessor systems as analyzed by different authors. König et al,18 in their comparative analysis of aneurysms treated with the WEB 17 versus the WEB 21 system, found that the WEB 17 expands the treatment indications toward smaller and more distally located aneurysms with a similar and, to some extent, lower complication rate. These findings are in line with those of Goertz et al,19 who found a potentially lower thromboembolic event rate without compromising the initial occlusion rate with the WEB 17.
Endovascular coiling of small and very small (≤3.0 mm) aneurysms is challenging compared with larger aneurysms. This issue is mainly related to the higher risk of rupture caused by an unexpected movement of the microcatheter.20,21 Endovascular coiling of aneurysms of ≤3.0 mm is more prone to failure compared with larger aneurysms following a study of Pierot et al.22 Compliant balloons or stents are helpful tools to increase the packing density in smaller aneurysms, while balloons are further useful devices in cases of an acute aneurysm rupture.20,23,24 However additional devices are associated with a higher periprocedural complication rate in small aneurysms, and recanalization rates were found to be higher in the group of stent-assisted coiling of small aneurysms according to the meta-analysis of Yamaki et al.21
The results of ours and previous studies underline the effectiveness of the WEB 17 in the treatment of small (atypically located) broad-based aneurysms, which is primarily related to the softness of the device, which might reduce the incidence of intraprocedural ruptures. Furthermore, does the “single device concept” compared with remodeling or stent-assisted coiling potentially reduce procedure time and with this the probability of adverse events.
Limitations
Our study has limitations that are mainly the consequence of the retrospective nature, without a stringent definition of inclusion and exclusion criteria. Furthermore, the angiographic results were graded without an independent assessment, and only midterm follow-up data are available to date. However, to the best of our knowledge, this is the largest series of aneurysms in alternative locations treated with the WEB 17 device.
CONCLUSIONS
Treatment of aneurysms with the WEB 17 in locations different from those included in the GCP trials is safe and effective. Our results represent a further step toward an expansion of indications for intrasaccular flow disruption. Additional studies are needed to define the ideal indication for the WEB 17 system in alternative locations among the existing potential treatment options.
Footnotes
Disclosures: Christoph Maurer—UNRELATED: Grants/Grants Pending: Stryker/MicroVention, Comments: travel grants. Ansgar Berlis—RELATED: Consulting Fee or Honorarium: proctor for MicroVention; UNRELATED: Consultancy: proctor for Stryker; Payment for Lectures Including Service on Speakers Bureaus: Penumbra, Medtronic; phenox. Werner Weber—RELATED: Consulting Fee or Honorarium: proctor for MicroVention; UNRELATED: Consultancy: proctor for Stryker; Payment for Lectures Including Service on Speakers Bureaus: Penumbra, Medtronic; phenox. Sebastian Fischer—RELATED: Consulting Fee or Honorarium: consulting and proctoring agreement for MicroVention*; UNRELATED: Consultancy: agreement with Stryker, Phenox, RapidMedical. *Money paid to the institution.
References
- Received June 26, 2020.
- Accepted after revision October 12, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CLinical EValuation of WEB 17 device in intracranial aneuRysms (CLEVER): 1-year effectiveness results for ruptured and unruptured aneurysms
- CLinical EValuation of WEB 17 device in intracranial aneuRysms (CLEVER): procedural, 30-day and 1-year safety results for ruptured and unruptured aneurysms
- Aneurysm Treatment with Woven EndoBridge-17: Angiographic and Clinical Results at 12 Months from a Retrospective, 2-Center Series
- Use of the Woven EndoBridge Device for Sidewall Aneurysms: Systematic Review and Meta-analysis
- Intracranial aneurysm treatment with intrasaccular flow disruption: comparison of WEB-21 and WEB-17 systems