
Abstract
BACKGROUND AND PURPOSE: The aspiration technique has gained a prominent role in mechanical thrombectomy. The thrombectomy goal is successful revascularization (modified TICI ≥ 2b) and first-pass effect. The purpose of this study was to evaluate the impact of the vessel-catheter ratio on the modified TICI ≥ 2b and first-pass effect.
MATERIALS AND METHODS: This was a retrospective, single-center, cohort study. From January 2018 to April 2020, 111/206 (53.9%) were eligible after applying the exclusion criteria. Culprit vessel diameters were measured by 2 neuroradiologists, and the intraclass correlation coefficient was calculated. The receiver operating characteristic curve was used for assessing the vessel-catheter ratio cutoff for modified TICI ≥ 2b and the first-pass effect. Time to groin puncture and fibrinolysis were weighted using logistic regression. All possible intervals (interval size, 0.1; sliding interval, 0.01) of the vessel-catheter ratio were plotted, and the best and worst intervals were compared using the χ2 test.
RESULTS: Modified TICI ≥ 2b outcome was achieved in 75/111 (67.5%), and first-pass effect was achieved in 53/75 (70.6%). The MCA diameter was 2.1 mm with an intraclass correlation coefficient of 0.92. The optimal vessel-catheter ratio cutoffs for modified TICI ≥ 2b were ≤1.51 (accuracy = 0.67; 95% CI, 0.58–0.76; P = 0.001), and for first-pass effect, they were significant (≤1.33; P = .31). The modified TICI ≥ 2b odds ratio and relative risk were 9.2 (95% CI, 2.4–36.2; P = 0.002) and 3.2 (95% CI, 1.2–8.7; P = .024). The odds ratio remained significant after logistic regression (7.4; 95% CI, 1.7–32.5; P = .008). First-pass effect odds ratio and relative risk were not significant (2.1 and 1.5; P > .05, respectively). The modified TICI ≥ 2b best and worst vessel-catheter ratio intervals were not significantly different (55.6% versus 85.7%, P = .12). The first-pass effect best vessel-catheter ratio interval was significantly higher compared with the worst one (78.6% versus 40.0%, P = .03).
CONCLUSIONS: The aspiration catheter should be selected according to culprit vessel diameter. The optimal vessel-catheter ratio cutoffs were ≤1.51 for modified TICI ≥ 2b with an odds ratio of 9.2 and a relative risk of 3.2.
ABBREVIATIONS:
- ADAPT
- a direct aspiration first‐pass technique
- mTICI
- modified TICI
Stroke represents the second leading cause of death in the world;1 however, the case fatality rate has decreased in recent decades due to primary prevention and treatment improvements.2 After the introduction in various guidelines,3,4 patients treated with mechanical thrombectomy showed a significant decrease of disability at 90 days compared with controls (OR = 2.49; 95% CI, 1.76–3.53; P < .0001)5 and a reduction of decompressive hemicraniectomy for malignant cerebral edema (range, 11.4%–4.8%; P < .001).6 Recently, a direct aspiration first-pass technique (ADAPT) has gained a level of I B-R for mechanical thrombectomy in the 2019 guidelines for stroke management.3 An modified TICI (mTICI) of grade 2b/3 is the mechanical thrombectomy goal for increasing good functional outcome;3,7 in addition, first-pass effects have earned a prominent role in stroke prognosis.8
Nikoubashman et al9 demonstrated, in an experimental animal study, that large-bore catheters should have an inner diameter of >1.016 mm for the MCA and >1.524 mm for the ICA. Moreover, Alawieh et al10 showed a higher rate of recanalization and first-pass effect using larger diameter catheters versus smaller ones (ACE64/ACE68 [Penumbra] versus 5MAX ACE [Penumbra], 85%/81% versus 61%, P < .05, respectively). However, no differences were found in terms of first-pass effect, reperfusion, and clinical outcome among different large-bore catheters selected (Catalyst 6, Stryker; Sofia, MicroVention; Navien, Covidien; ACE68, Penumbra; P > .05).11
The aim of this study was to evaluate the impact of the vessel-catheter ratio on successful revascularization and first-pass effect in a tertiary center (Azienda Ospedaliera San Camillo/Forlanini) for cerebrovascular disease treatment.
MATERIALS AND METHODS
This study was approved by the ethics institutional review board. Informed consent was waived due to the retrospective nature of this study.
The manuscript was drafted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.12
This was a retrospective, single-arm, single-center, cohort study. From January 2018 to April 2020, we evaluated all patients admitted to the stroke unit of a tertiary hub center who underwent endovascular thrombectomy according to current guidelines.3 The exclusion criteria for the study were the following: non-MCA and mechanical thrombectomy technique different from ADAPT. Because there is no definitive indication regarding which endovascular technique should be used for thrombectomy,3 the choice was left to the interventional neuroradiologist at the time of the procedure. The clinical details of the cohort are given in Table 1.
Clinical details
Technical success was defined with a mTICI 2b or 3.3,4 The first-pass effect would be mTICI ≥ 2b in 1 passage of the catheter.
The vessel-catheter ratio was calculated as the fraction between the culprit vessel and the inner diameter of the catheter used for aspiration because the inner diameter is the “active” part for aspiration force.13
Vessel-Diameter Measurement
The diameter of the occluded vessel was measured by 2 neuroradiologists (S.F. and L.B. with 20 and 8 years of experience, respectively) in the straight tract of the closest vessel before the thrombus on DSA.14 The simple mean between these measurements was taken for further analysis, and the intraclass correlation agreement was calculated.
Endovascular Technique
All patients were treated using ADAPT by 5 experienced neurointerventional radiologists (>7 years’ experience) in a dedicated angiosuite (biplane Artis zee; Siemens).
All procedures were performed via arterial access with the patient under sedation or general anesthesia according to the present clinical status and stroke severity. ADAPT was performed through femoral access using a 6F long vascular sheath (Neuro MAX 088, Penumbra; or AXS Infinity LS, Stryker Neurovascular) positioned in the ICA of the culprit side. The size of the intermediate aspiration catheters was chosen by the neurointerventional radiologist at the time of the procedure; in 1/111 (0.9%), a distal aspiration catheter was used. The intermediate catheters used were both Stryker and Penumbra systems and were divided according to their inner diameter into the following: 1.37 mm (5MAX ACE), 1.47 mm (AXS Catalyst 5; Stryker), 1.52 mm (AXS Catalyst 6), 1.62 mm (AXS Catalyst 7), 1.63 mm (ACE64), and 1.73 mm (ACE68). The distal aspiration catheter used has an inner distal lumen of 1.09 (3MAX; Penumbra). The ADAPT was always performed without a microguidewire inside the lumen and with an aspiration pump (Pump MAX; Penumbra).9 See Table 2 for frequency.
Technical details
Study Outcome
The primary outcome was to evaluate the cutoff value of the vessel-catheter ratio, maximizing the likelihood of obtaining mTICI ≥ 2b. Furthermore, the impact on successful revascularization of the adequate vessel-catheter ratio was weighted with fibrinolysis and time to groin puncture. Subanalysis was performed for first-pass effect versus a control group (non-first-pass effect revascularization + mTICI ≤ 2a). The secondary outcome was to evaluate the impact of different cutoff values on the likelihood of obtaining a successful revascularization and a first-pass effect.
Data Base Preparation
Clinical data were retrospectively derived from a prospective data base drafted by the stroke unit. The radiologic parameters were evaluated through Radiology and Imaging Specialists/PACS systems by 1 neuroradiologist (5 years of experience) not involved in the procedure. The angiographic measurements of culprit vessel diameter were evaluated by 2 neuroradiologists, and the simple mean was taken for the analysis.
Statistical Analysis
Normality was tested using the Kolmogorov-Smirnov Z, and continuous variables were reported accordingly. Ordinal values were reported as percentages. The intraclass correlation coefficient (for vessel diameter) was calculated using the intraclass correlation. mTICI was defined dichotomously in successful (mTICI ≥ 2b) and unsuccessful (mTICI ≤ 2a) revascularization. The receiver operating characteristic curve and Youden index were used for assessing the optimal cutoff values for the vessel-catheter ratio. The odds ratio, the relative risk, and the number of patients to be treated were calculated. Logistic regression was used for analyzing the impact on successful revascularization of the vessel-catheter-ratio, fibrinolysis, and time to groin puncture The impact of different cutoff values of the vessel-catheter ratio was evaluated by calculating the percentage of successful revascularizations and first-pass effects using an interval of 0.1 and an interval increment of 0.01, starting at the lowest value of the vessel-catheter ratio (1.0) to the highest (1.7); subsequently, the percentage was plotted. For both analyses, a subgroup evaluation was performed using first-pass effect as endpoint. Statistical analysis was performed, and the graph was plotted using MedCalc 18.2.1 (MedCalc Software) and Excel (Microsoft). P values < .05 were considered statistically significant, and all P values were calculated using a 2-tailed significance level.
RESULTS
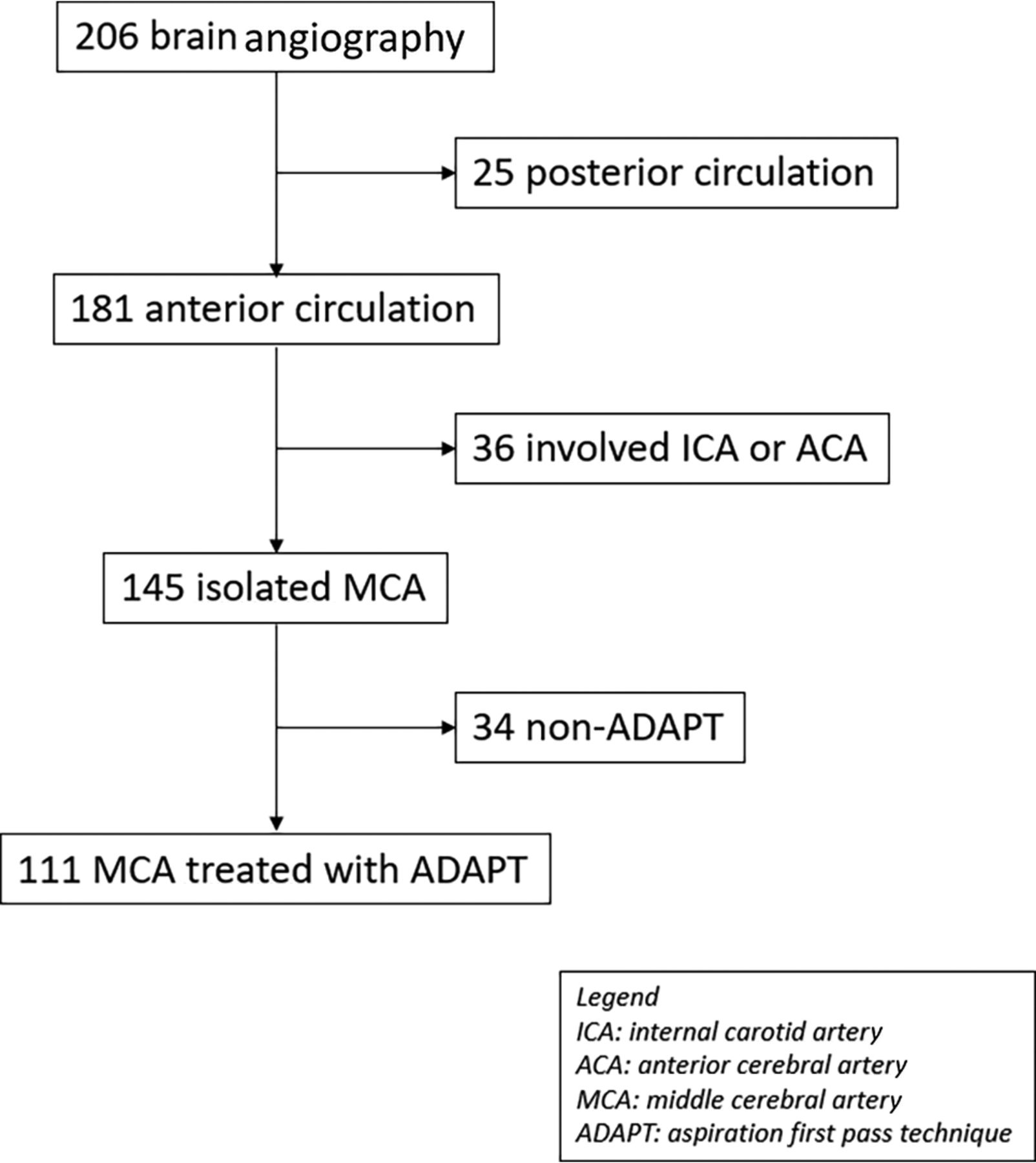
Two-hundred six consecutive patients underwent brain angiography for mechanical thrombectomy; after applying the exclusion criteria, 95/206 (46.1%) were further excluded from the analysis. Thirty-six of 95 (37.9%) of the strokes involved the ICAs, 25/96 (26.3%) had posterior circulation stroke, and in 34/95 (35.8%) ADAPT was not used as the first-line technique. The final population encompassed 111/206 (53.9%) patients with MCA stroke treated with ADAPT; the clinical details are provided in Table 1. Twenty-three of 111 (20.7%) were wake-up strokes. The flowchart of the study is shown in Fig 1. The rate of mTICI ≥ 2b was 75/111 (67.5%), and the first-pass effect was 53/75 (70.6%). All patients with mTICI ≤2a (36/111 [32.5%]) underwent a rescue technique. The median vessel diameter was 2.1 mm (95% CI, 2.0–2.1; range, 1.3–3.9; mean, 2.1 [SD, 0.4]); the intraclass correlation coefficient was 0.92 (95% CI, 0.84–0.97). Technical parameters are shown in Table 2.

Study flow chart.
The optimal vessel-catheter ratio cutoff for maximizing the likelihood of obtaining mTICI ≥ 2b was ≤1.51 (accuracy = 0.67; 95% CI, 0.58–0.76; P = 0.001). With a vessel-catheter ratio of ≤1.51 as a cutoff, the chances of obtaining mTICI ≥ 2b were significantly higher compared with the vessel-catheter ratio of >1.51 (OR, 9.2; 95% CI, 2.4–36.2; P = 0.002; relative risk, 3.2; 95% CI, 1.2–8.7; P = 0.02). The number of patients to be treated to observe a benefit with a vessel-catheter ratio of ≤1.51 was 2.0 (95% CI, 1.3–4.0). The likelihood of achieving successful revascularization also remained significant after logistic regression both for all patients and for those with non-wake up stroke (OR = 9.6; 95% CI, 2.4–38.7; P = .0014; OR = 7.3; 95% CI, 1.7–32.1; P = .008, respectively) (see Tables 3 and 4 for details). No significant cutoff was found for first-pass effect likelihood as outcome, though the highest Youden index was for vessel-catheter ratio of ≤1.33 (accuracy = 0.56; 95% CI, 0.46–0.65; P = .31). With the vessel-catheter ratio of ≤1.33, there was a trend toward first-pass effect likelihood, although not statistically significant (OR = 2.1; 95% CI, 0.93–5.0; P = .07 with a relative risk of 1.5; 95% CI, 0.93–2.5; P = .10, respectively). The ORs of logistic regression analysis were not statistically significant either (Tables 3 and 4).
Successful revascularization (mTICI ≥ 2b)a
First-pass effect
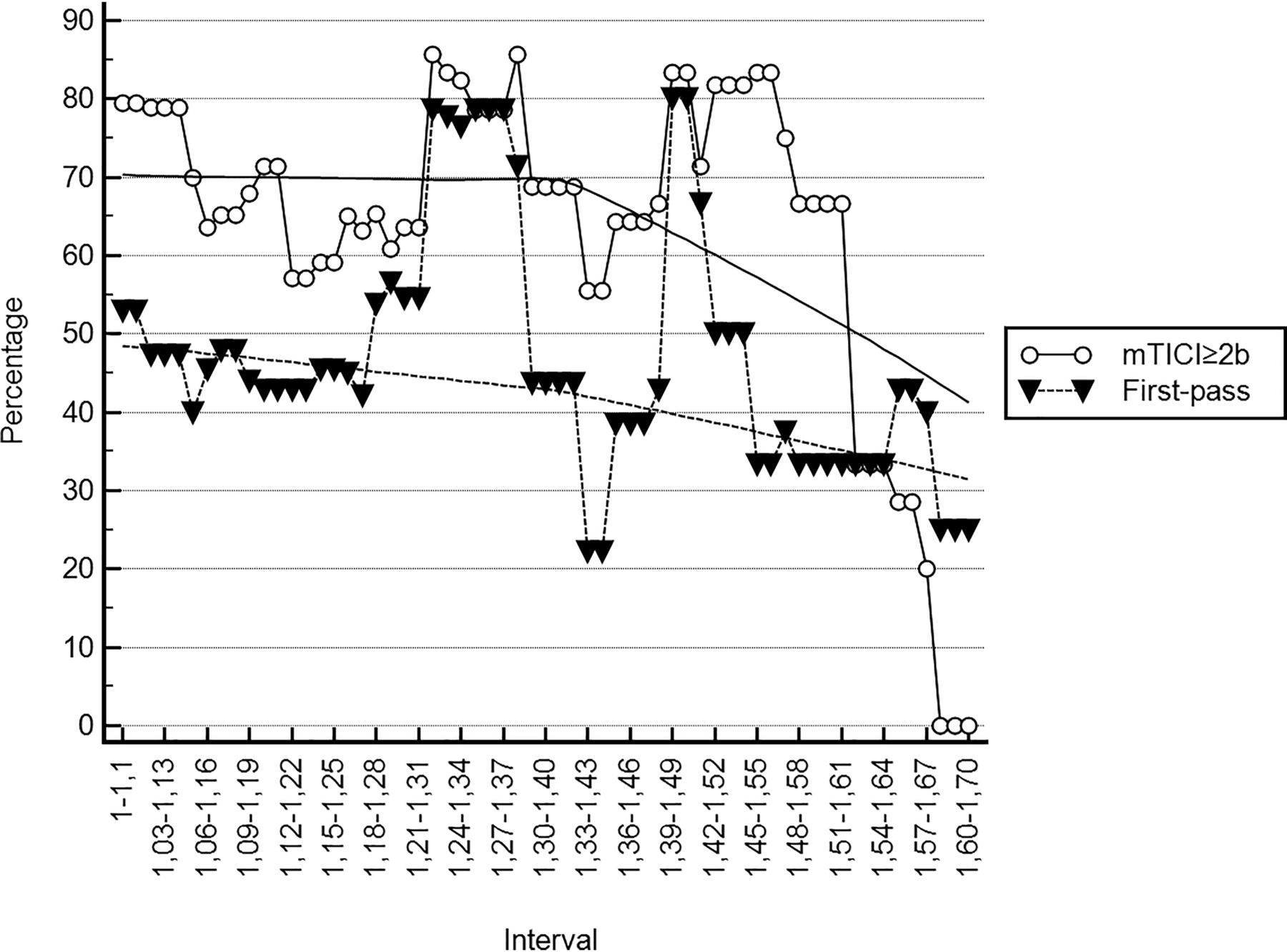
The percentage of successful revascularizations of the 0.1 interval ranged from 0.0% to 85.7% (median, 66.7%; 95% CI, 64.6%–70.0%). Considering exclusively the interval below 1.51, the percentage ranged from 55.6% to 85.7% (median 68.8%; 95% CI, 65.0%–71.4%). No statistically significantly differences were found between the percentage of the worst interval (1.34–1.44) and the best one (1.28–1.38; 55.6% versus 85.7%; P = .12, respectively) (Fig 2). The percentage for obtaining a successful revascularization in 1 passage ranged from 0.0% to 80.0%; considering the interval below 1.33, the percentage ranged from 40.0% to 78.6% (median, 47.4%; 95% CI, 44.7%–52.9%). The percentage for obtaining first-pass revascularization of the best interval (range, 1.26–1.36) was significantly higher compared with the worst one (range, 1.05–1.15; 78.6% versus 40.0%; P = .03, respectively) (Fig 2).

The plot shows the trend of successful revascularization (line with dot) and a first-pass effect (dotted line with triangle) together with the tendency line among different intervals of vessel-to-catheter ratios. As observed, after the respective cutoff (≤1.51 and ≤1.33) for mTICI ≥ 2b and first-pass effect, the trend remains stable.
DISCUSSION
The best cutoff of the vessel-catheter ratio to maximize the likelihood for achieving mTICI ≥ 2b was ≤1.51 (accuracy = 0.67, P = .0012, OR = 9.2), with a percentage of successful revascularization spanning 55.6% to 85.7% (vessel-catheter ratio interval, 1.0–1.51). For the first pass, the optimal cutoff, though not statistically significant, was 1.33 (accuracy = 0.56, P = .31, OR = 2.1), with a range of first-pass effect from 40.0% to 78.6% (vessel-catheter ratio interval, 1.0–1.33).
Different companies tried to increase the diameter of large-bore catheters (from 1.37 to 1.82 mm)15 for ADAPT, based on the assumption that “the bigger the catheter is, the better the result will be,” with the lessening of maneuverability for larger catheters.9 This paradigm is supported by the concept that a larger inner diameter increases the aspiration flow rate and therefore the likelihood of thrombus aspiration.13 These results are supported by the present study, which showed a cutoff of the vessel-catheter ratio for reaching mTICI ≥ 2b of ≤1.51 with an OR = 9.2 (95% CI, 2.4–36.2) and a number of patients treated of 2.0 (95% CI, 1.3–4.0). Despite the wide 95% CI, this result remained significant after considering the time to groin puncture and fibrinolysis (Table 3). Most interesting, in the interval of the vessel-catheter ratio between 1.0 and 1.51, the percentage of successful revascularizations ranged from 55.6% to 85.7% without statistically significantly differences (Fig 2). This finding apparently contradicted the above-mentioned axiom; however, probably, once a sufficient aspiration force was achieved,16 the following increment did not increase the chance of thrombus removal. Thus, the catheter should be selected according to vessel diameter, keeping in mind reaching at least a vessel-catheter ratio of ≤1.51. The ADAPT axiom should move from “the bigger the better” to “the fitter the better.”
First-pass effect is a known favorable prediction factor for ischemic stroke recovery (OR = 2.4–3.2).8,17 Large-bore catheters increased the rate of first-pass effect in an ADAPT series (53% versus 33%, P = .04), and the ACE68 was an independent predictor of successful reperfusion and good clinical outcome (OR = 1.67 and 6.2, respectively).18 Although not significant, a statistical trend for first-pass effect was found with a vessel-catheter ratio of ≤1.33 (accuracy = 0.56; 95% CI, 0.46-0.65; P = .31) and an OR = 2.1 (95% CI, 0.93–5.0; P = .07). Considering the interval between 1.0 and 1.33, the percentage of first-pass effect ranged from 40.0% to 78.6%, superior to all of cases in the Contact Aspiration vs Stent Retriever for Successful Revascularization (ASTER) trial subanalysis (26.3%),18 and in line with the results of Delgado Almandoz et al (53%).19 This discrepancy may be explained by the unknown vessel-catheter ratio in these studies. In fact, a significantly better first-pass effect prevalence was found in the best interval (1.26–1.36) compared with the worst one (1.05–1.15; 78.6% versus 40.0%; P = .03) (Fig 2).
The reported mean diameter of the MCA is 2.3 mm, which is similar to our finding of 2.1 (SD, 0.4) mm.14 Setting a vessel-catheter ratio of ≤1.51 (cutoff for mTICI ≥ 2b) and considering the reported diameter of 2.3 mm, the minimum catheter inner diameter was 1.5 mm.
Our study had several limitations. First, this was a single-center, nonrandomized study with a control group. Second, the large-bore catheters used were mostly Catalyst 6 (26.1%) and ACE68 (64.0%). Third, the sample size was low, especially for a first-pass effect, as shown by the large 95% CI of our findings, though the number of patients (n = 111) was in line with those in monocentric stroke studies.
CONCLUSIONS
The catheter selection for ADAPT should be performed keeping in mind the goal of a vessel-catheter ratio of ≤1.51 for increasing to mTICI ≥ 2b. For achieving mTICI ≥ 2b, considering the average diameter of middle cerebral artery, the inner diameter of the intermediate catheter should be ≥1.5 mm.
Footnotes
Disclosures: Gianluca De Rubeis—UNRELATED: Employment: Sapienza University of Rome. Claudio Gasperini—UNRELATED: Board Membership: Merck, Bayer AG, Teva Pharmaceutical Industries, Biogen, Novartis, Roche, Almirall, Sanofi; Payment for Lectures Including Service on Speakers Bureaus: Merck, Bayer AG, Teva Pharmaceutical Industries, Biogen, Novartis, Roche, Almirall, Sanofi; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Merck, Bayer AG, Teva Pharmaceutical Industries, Biogen, Novartis, Roche, Almirall, Sanofi.
References
- Received July 20, 2020.
- Accepted after revision October 5, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tenzing Assisted Delivery of Aspiration (TADA) technique for thrombectomy of medium vessel occlusions using the Freeclimb 54 catheter: multicenter experience
- In Vitro Analysis of the Efficacy of Endovascular Thrombectomy Techniques according to the Vascular Tortuosity Using 3D Printed Models
- Comparison of aspiration versus combined technique as first-line approach in terminal internal carotid artery occlusion: a multicenter experience