
Abstract
BACKGROUND AND PURPOSE: The efficacy of mechanical thrombectomy methods may differ depending on the characteristics of the occlusion. The purpose of this study was to compare the recanalization efficacy and treatment outcome of a stent retriever versus contact aspiration in patients with acute basilar artery occlusion according to the angiographic characteristics of the occlusion.
MATERIALS AND METHODS: One hundred sixty-one patients with acute basilar artery occlusion who underwent mechanical thrombectomy were retrospectively analyzed. A stent retriever was compared with contact aspiration thrombectomy according to the clot meniscus sign, defined as a meniscoid/tram-track-like sidewall contrast opacification of the thrombus. A propensity score matching analysis was performed. Clinical/angiographic characteristics and treatment and clinical outcomes were compared.
RESULTS: Overall, a stent retriever (n = 118) and contact aspiration (n = 43) did not show significant differences in the successful recanalization (82.2% versus 86.0%) and good clinical outcome rates (32.2% versus 39.5%). In patients with the positive meniscus sign, contact aspiration was associated with shorter procedural time (44 versus 26 minutes, P = .018), a lower number of passes (2 versus 1, P = .041), a higher complete recanalization rate (58.8% versus 85.7%, P = .021), and a higher rate of first-pass effect (27.9% versus 53.6%, P = .031) compared with a stent retriever. After propensity score matching, contact aspiration was associated with higher complete recanalization rates (59.3% versus 85.7%, P = .033). No significant differences in the outcomes were noted between a stent retriever and contact aspiration in patients negative for the meniscus sign.
CONCLUSIONS: The efficacy of the mechanical thrombectomy techniques may differ according to the angiographic characteristics of occlusion in patients with basilar artery occlusion. Contact aspiration may be more effective in terms of recanalization compared with a stent retriever in patients with the clot meniscus sign.
ABBREVIATIONS:
- BAO
- basilar artery occlusion
- CA
- contact aspiration
- MT
- mechanical thrombectomy
- PSM
- propensity score matching
- SR
- stent retriever
Randomized controlled trials have shown the safety and efficacy of mechanical thrombectomy (MT) in patients with acute ischemic stroke due to intracranial large-vessel occlusion.1
The 2 most widely used concepts of MT are a stent retriever (SR) and contact aspiration (CA). Recent randomized trials have demonstrated comparable efficacy between the SR and CA techniques as first-line thrombectomy approaches in the anterior circulation.2,3 However, little is known about the differences in the efficacy of the MT methods in terms of the angiographic characteristics of the occlusion. The differences in the anatomy of the occlusion between the anterior and posterior circulation may also cause different efficacies of MT techniques.
Angiographic morphology of the occlusive lesion may be an imaging biomarker reflecting the characteristics of the occlusion. Some previous studies have shown that the efficacy of MT methods may be influenced by the nature of the occlusion suggested by its angiographic morphologic features.4⇓⇓-7 A clot meniscus sign is a descriptive angiographic finding of meniscoid or sidewall opacification at the occlusion site, suggesting an embolic mechanism rather than an intracranial atherosclerosis-related occlusion.4,8
We hypothesized that the clot meniscus sign could be associated with a differential response according to the MT technique in patients with posterior circulation stroke. Therefore, we aimed to compare the recanalization efficacy and treatment outcomes of an SR versus CA according to the presence of the clot meniscus sign in patients with basilar artery occlusion (BAO).
MATERIALS AND METHODS
Patients
Data were collected from prospective registries of 2 tertiary university hospitals. From the registries, all consecutive acute patients with BAO referred for MT between March 2013 and December 2019 were enrolled. This study was conducted with the approval of the institutional review boards, which waived the need for written informed consent because of the retrospective nature of the study.
Both centers used the following inclusion criteria: 1) acute symptomatic patients with BAO identified on CT or MR angiography, 2) time from onset of symptoms to groin puncture of ≤12 hours, 3) a baseline NIHSS score of equal or more than four, 4) no intracranial hemorrhage detected on initial CT, and 5) patients having undergone MT using SR or CA thrombectomy as the primary treatment. Exclusion criteria were the following: 1) BAO due to other causes such as arterial dissection, vasculitis, or Moyamoya disease; 2) thrombolysis as first-line endovascular therapy or navigation failure; and 3) poor quality of the angiography image for review. Part of the patient cohort was included in a prior study examining the overall significance of the clot meniscus sign.4
Image Analysis
The imaging findings were investigated by 2 interventional neuroradiologists in consensus (D.J.K. and S.H.B. with 18 and 4 years of experience, respectively). The reviewers were blinded to the clinical outcome during image analysis. The clot meniscus sign was defined as a meniscoid/edge-like appearance at the proximal occlusion site or a tram-track-like appearance and antegrade sidewall contrast opacification distal to thrombus on the arterial phase image of the presenting initial angiography. All other findings such as fading/tapering and abrupt cutoff were considered as absence of the clot meniscus sign.4 The angiographic assessment of the clot meniscus sign was based on cerebral angiographic images, which were selected from the arterial phase with best vessel contrast filling. Both centers used the same standard DSA machine (Allura Xper FD 20/20; Philips Healthcare).
The location of the BAO was divided into proximal (from the vertebrobasilar junction to the origin of the anterior inferior cerebellar artery), middle (from the origin of the anterior inferior cerebellar artery to the origin of the superior cerebellar artery), and distal occlusion (distal to the origin of the superior cerebellar artery) according to the cerebral angiography findings.9
Endovascular Treatment
All included patients were treated with MT using either the SR or CA technique. The patients were divided into SR and CA groups on the basis of the first-line MT technique used. All endovascular procedures were performed by 3 interventional neuroradiologists (D.J.K., B.M.K., and C.J., with 18, 17, and 12 years of experience, respectively). Before the procedure, the CTA images were reviewed for evaluation of the site of the occlusion and the access route. In general, the procedure was performed via the femoral approach using a 6F shuttle sheath and/or a 5F or 6F guiding/intermediate catheter for access to the vertebral artery.
The first-line MT approach was chosen at the operator’s discretion. SR thrombectomy was performed using a stent retriever device (Solitaire FR, Covidien; Trevo, Stryker) with or without the use of an intermediate catheter (n = 29, Sofia or Sofia Plus, MicroVention; AXS Catalyst, Stryker Neurovascular; Navien, Medtronic). When an SR was used as the first-line device, the case was classified as the SR group irrespective of concomitant intermediate catheter use. The intermediate catheter in these cases was mostly placed in the distal vertebral artery and used for support during microcatheter navigation. CA thrombectomy was performed using a large-bore aspiration catheter (Penumbra System Reperfusion Catheter; Penumbra) or an intermediate catheter. If successful reperfusion was not achieved with the initially selected first-line approach despite multiple attempts, rescue therapy was performed by switching to another strategy. A balloon-guiding catheter for proximal flow control was not used in any cases. The details of the techniques used for an SR or CA for BAO have been described previously.10
Outcome Measures
Clinical and radiologic data regarding patient demographics, angiographic findings, and time intervals (ie, onset, puncture, recanalization time) were prospectively collected. The procedural time was defined as the interval from puncture to final recanalization in successful recanalization and from the time of the last angiographic series in patients with unsuccessful recanalization. Recanalization status was assessed on the final angiogram and was classified according to the modified TICI scale: Successful recanalization was defined as modified TICI grades 2b or 3, and complete recanalization was defined as modified TICI grade 3. First-pass effect was defined as achieving complete recanalization with a single thrombectomy device pass. Good clinical outcome was defined as a 90-day mRS score of 0–2. All neurologic examinations were performed by board-certified neurologists. The patients were routinely evaluated for determination of the stroke etiology, which included echocardiography, continuous electrocardiography monitoring in a stroke unit or Holter monitoring, and cardiac CT.
The adverse events of interest included procedural complications (vessel perforation and dissection), hemorrhagic complications, and any cause of mortality at 90 days. A nonenhanced brain CT or MR imaging was routinely performed in the first 24 hours after the procedure. An intracerebral hemorrhage was classified according to the Second European-Australasian Acute Stroke Study classification, and symptomatic intracerebral hemorrhage was defined as any hemorrhage associated with an NIHSS score increase of ≥4 within 24 hours.11
Statistical Analysis
The baseline characteristics and clinical outcomes between patients treated with SR and CA first-line thrombectomy were compared (SR versus CA groups). The treatment and clinical outcomes between the SR and CA groups were also compared according to the presence of the clot meniscus sign. To reduce data bias and confounding variables, we performed the propensity score matching (PSM) analysis by matching patients in the 2 groups at a 1:1 ratio according to nearest neighbor matching algorithm. The covariates used to generate these propensity scores included age, sex, hypertension, diabetes, dyslipidemia, smoking, coronary artery disease, baseline NIHSS score, intravenous tPA, the clot meniscus sign, and onset-to-puncture time.
In the overall sample, the Pearson χ2 test or Fisher exact test was used for categoric variables, and the Mann-Whitney U test, for comparison of continuous variables. In the PSM sample, the McNemar test was used for categoric variables, and the Wilcoxon singed-rank test, for comparison of continuous variables. Multivariable logistic regression was performed to evaluate the independent variables for complete recanalization in patients with the clot meniscus sign. A P value < .05 was considered statistically significant. Statistical analyses were performed using SPSS for Windows (Version 20.0; IBM) and R statistical and computing software (Version 3.6.2; http://www.r-project.org/).
RESULTS
During the study period, 281 patients who underwent MT for acute BAO were initially enrolled. Among them, 186 patients who met the inclusion criteria were included. Of these, 25 patients were excluded due to the following: intra-arterial thrombolysis as a first-line method (n = 8), occlusion due to dissection (n = 9) or vasculitis (n = 3), and poor quality of the angiography for review (n = 5). The remaining 161 (median age 73 years; interquartile range, 66–80 years; 94 men [58.4%]) patients were finally enrolled in the present study. A total of 118 (73.3%) of the 161 patients were treated with an SR as the first-line thrombectomy (SR group), and 43 (26.7%) patients were treated with CA as the first-line thrombectomy (CA group). After PSM, 43 patients in each group were matched (Fig 1).

Flow chart of patient selection. NIHSS indicates National Institutes of Health Stroke Scale; IA, intra-arterial; SR, stent retriever; CA, contact aspiration.
The baseline characteristics and treatment outcomes of the overall and PSM samples between the 2 groups are shown in the Online Supplemental Data. Overall, the median baseline NIHSS score was 16 (interquartile range, 8–25) in the SR group and 21 (interquartile range, 11–25) in the CA group (P = .438). There were no statistically significant differences in the successful recanalization (82.2% versus 86.0%) and good clinical outcome rates (32.2% versus 39.5%), but CA was associated with a shorter procedural time (56 versus 33 minutes, P = .009), fewer passes (3 versus 1, P = .001), higher complete recanalization rates (47.5% versus 69.8%, P = . 012), higher first-pass effect (19.5% versus 39.5%, P = . 009), and a lower symptomatic intracerebral hemorrhage rate (11.0% versus 0%, P = .021). Three cases of vessel perforation were identified in the patients treated with an SR. The vessel perforations occurred at the basilar artery perforator (n = 2) and the P1–2 segments (n = 1). In the latter case, coil embolization was performed at the proximal parent artery due to continued contrast leakage. All patients with vessel perforation showed poor clinical outcome. There were 3 cases (7.0%) of iatrogenic vertebral artery dissection at the V2 segment in the CA group. Two patients underwent stent placement for management of the dissection and had poor clinical outcomes. One patient was treated with 0.5 mg of intra-arterial tirofiban and did not show flow impairment or thrombus formation on the delayed angiogram. This patient had a good clinical outcome. After PSM, the CA group was associated with a lower number of passes (median, 3 versus 1; P = .045). Other baseline factors did not show any significant differences between the 2 groups.
The treatment and clinical outcomes according to the presence of the clot meniscus sign are summarized in the Online Supplemental Data. The clot meniscus sign was seen in 59.6% (96/161) of patients. In the patients positive for the meniscus sign, the CA group showed a shorter procedural time (44 versus 26 minutes; P = .018), a lower total number of passes (median, 2 versus 1; P = .041), a higher rate of complete recanalization (58.8% versus 85.7%; P = .021), and a higher rate of first-pass effect (27.9% versus 53.6%; P = .031) compared with the SR group (Fig 2). After PSM, the CA group was associated with a higher complete recanalization rate (59.3% versus 85.7%, P = .033) and a tendency toward a higher first-pass effect (29.6% versus 53.6%, P = .084). No significant differences in the outcomes were noted between the SR and CA groups in the patients negative for the meniscus sign except for the shorter procedural time in patients with PSM and CA (90 versus 56 minutes, P = .02).

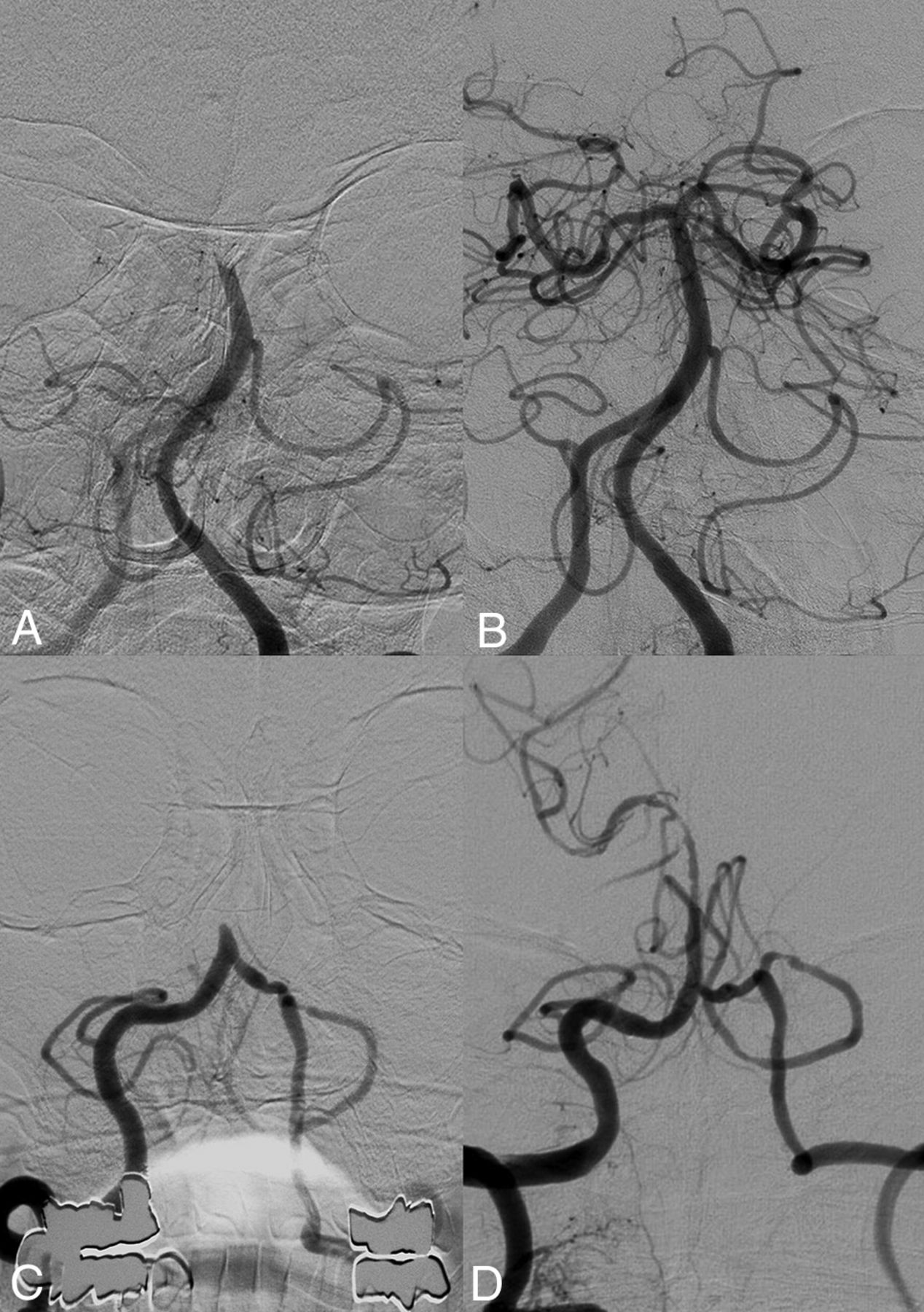
Pre- (A) and post- (B) thrombectomy images of a basilar artery occlusion in a patient with the positive clot meniscus sign. Complete recanalization was achieved using a single attempt of contact aspiration. Pre- (C) and post- (D) thrombectomy images of a patient with a basilar artery occlusion with the negative clot meniscus sign. Following an unsuccessful first-line approach with contact aspiration, multiple attempts of rescue thrombectomy were performed with the stent retriever, revealing an underlying atherosclerotic stenosis (not shown). Recanalization was achieved by permanent stent placement.
Multivariate logistic regression analysis showed that procedural time (OR, 0.96; 95% CI, 0.94–0.98; P = .001) and CA thrombectomy (OR, 7.09; 95% CI, 1.33–37.85; P = .022) were independent predictors of complete recanalization in patients with the positive clot meniscus sign when adjusting for age, hypertension, diabetes, baseline NIHSS score, intravenous tPA, distal BAO, onset-to-puncture time, number of passes, and the hospital (Table).
Multivariable analysis for complete recanalization in patients with a positive clot meniscus sign
DISCUSSION
The results of the present study showed that the clot meniscus sign in patients with posterior circulation stroke could be a discriminative imaging biomarker for predicting the recanalization efficacy of MT techniques. Patients with BAO with the clot meniscus sign treated with CA as the first-line approach exhibited a higher rate of complete recanalization, a shorter procedural time, and a higher rate of first-pass effect compared with those treated with SR thrombectomy. CA was an independent predictor of complete recanalization in patients with BAO with the clot meniscus sign.
Currently, CA is considered as noninferior to an SR as a primary MT modality for anterior circulation stroke.2,3,12 However, little is known about the association between the morphologic features of the occlusion and the preferred MT technique. Also, the posterior circulation differs from the anterior circulation in terms of anatomy, such as the caliber, tortuosity of the vessels, and the pattern of collaterals. These differences may alter the MT strategy such as forgoing the use of balloon-guide catheters. In the posterior circulation, stroke is also more frequently associated with in situ intracranial atherosclerotic stenosis than in the anterior circulation; this characteristic may also influence the efficacy of MT.10,13
There are mixed retrospective results and insufficient evidence supporting a specific technique for MT of acute BAO. Similar to the anterior circulation stroke, a few retrospective studies have reported that successful recanalization rates and clinical outcome did not differ significantly between the CA and SR devices for acute BAO,14⇓-16 whereas there have also been some reports demonstrating the superiority of CA over an SR in acute BAO. Selection of CA as the first-line MT achieved higher rates of complete recanalization with shorter procedural times compared with an SR in these studies.14,16,17
In terms of the morphologic features of the occlusion and the efficacy of MT methods, only a limited number of studies are available. Baik et al4 showed that the clot meniscus sign was a reliable imaging biomarker and predictor of successful recanalization in acute patients with BAO with excellent inter-/intrareader agreement. Yamamoto et al18 reported that the angiographic claw sign, thrombus that protruded proximally by more than half the diameter of the parent artery, is associated with successful recanalization after MT. Consoli et al5,6 and Kaiser et al7 showed that the regular thrombus morphology, a smooth and straight profile of the occlusion with a linear interruption of flow, was associated with better procedural and clinical outcomes when treated with CA compared with thrombus with irregular morphology, any kind of evident modification of the linearity of the occlusion, which seemed to show better results with an SR.
Our results showed that the recanalization efficacy is better with CA than an SR in patients with BAO with the positive clot meniscus sign. There may be several explanations for the superiority of CA over an SR. One reason could be the absence of proximal flow control in MT of posterior circulation strokes coupled with the embolic etiology of the occlusion in patients with the meniscus sign. In the anterior circulation MT studies, the use of a balloon-guide catheter is consistently associated with improved recanalization and clinical outcome.19⇓⇓-22 A balloon-guide catheter will reduce the impact force on the thrombus, allowing more effective retrieval, as well as minimizing the tendency for thrombus fragmentation and distal migration, but as in our study, it is rarely used in posterior circulation stroke due to collateral flow through the contralateral vertebral artery and the cervical arteries.23,24 Thus, a large-bore aspiration/intermediate catheter in the basilar artery during CA occupying a large percentage of the cross-sectional area of the vessel lumen can effectively decrease the impact force on the embolic clot, improving the recanalization efficacy.24 A recent study also showed the superiority of CA compared with an SR in achieving successful reperfusion for the treatment of terminal ICA occlusions in the absence of proximal flow arrest with balloon-guide catheters.25
In terms of the etiology of BAO, a previous study has shown that the positive clot meniscus sign was highly associated with distal BAO and an embolic etiology, whereas the negative clot meniscus sign was associated with proximal occlusion and arterial wall calcifications, suggestive of an underlying intracranial atherosclerotic stenosis.4 Imaging features similar to the meniscus sign such as the claw sign were also associated with the embolic etiology of the occlusion.18 Under these conditions, the action mechanism of CA may be more favorable than that of an SR. “Contact” between the tip of the aspiration catheter and proximal surface of the thrombus is the key technical element for achieving successful recanalization during CA thrombectomy.26 The meniscoid appearance of the occlusion may allow more area for contact with the aspiration catheter and also decrease the surface area interaction with the vessel wall, reducing friction/adhesion. With respect to SR thrombectomy, the key mechanism for effective thrombus removal is the integration of the SR device with the thrombus, which may be mostly determined by the histologic composition and consistency of the clot.27⇓-29 However, this relationship between the imaging morphology and the histologic clot composition/consistency has not been fully elucidated.
Last, in contrast to the SR technique in which a microcatheter is necessarily navigated across the clot, crossing the clot may be avoided, decreasing the risk of clot fragmentation, using the so-called “thrombus no-touch technique” in many cases of CA, especially with the relatively straight course of the basilar artery.30
In the meniscus sign–negative occlusions, the etiology of the BAO in many patients may have been due to an underlying intracranial atherosclerotic stenosis.4 intracranial atherosclerotic stenosis is known to be associated with lower rates of successful recanalization and poorer clinical outcomes with conventional MT techniques.10,31 Thus, these patients negative for the meniscus sign did not show a significant difference in treatment efficacy between an SR and CA in our series. Further research on specific imaging/clinical features for predicting optimal recanalization methods for these specific groups of patients is warranted.
There are several limitations to this study. First, due to the retrospective design, selection of the first-line MT device was at the discretion of the operator, resulting in potential bias. PSM was performed to reduce this potential bias between the 2 groups, and the superiority of CA was maintained in the patients positive for the meniscus sign. Another limitation in our study could be the lack of histologic examination of the retrieved clots. The relationship between the thrombus composition and the angiographic morphology could be a topic for future research.
CONCLUSIONS
The efficacy of the MT techniques may differ according to the angiographic morphology of the occlusion in patients with BAO. CA as the first-line MT approach may be more effective in terms of complete recanalization compared with an SR in patients with BAO with the clot meniscus sign. The clot meniscus sign may be used as an imaging biomarker for planning therapeutic strategies and maximizing procedural outcome.
Footnotes
This study was supported by a grant from the Research Institute of Radiological Science, Yonsei University College of Medicine (grant No. 4-2017-0877).
Disclosures: Dong Joon Kim—UNRELATED: Payment for Lectures Including Service on Speakers Bureaus: Stryker Pacific Limited.
References
- Received September 1, 2020.
- Accepted after revision November 3, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Can the clot meniscus and claw signs predict thrombectomy and clinical outcomes in patients with stroke? A systematic review and meta-analysis
- Aspiration only versus stent retriever only thrombectomy in basilar artery occlusion: a propensity score-matched analysis of the German Stroke Registry
- First-line contact aspiration versus first-line stent retriever for acute posterior circulation strokes: an updated meta-analysis