
Abstract
BACKGROUND AND PURPOSE: Various etiologies have been theorized for the development of congenital nasal pyriform aperture stenosis (CNPAS). Imaging possibly implicates abnormal fusion of the midline palatal suture and deficient lateral growth of the midface in affected neonates.
MATERIALS AND METHODS: A single-center, retrospective study was performed at a tertiary care pediatric hospital involving neonates and infants between 0 and 90 days of life. Maxillofacial CT scans of patients were reviewed. Abnormality of the palatal suture and midface transverse dimensions were measured and analyzed in patients with and without CNPAS.
RESULTS: A total of 109 patients between 0 and 90 days of life had maxillofacial CT scans. Thirteen patients were classified as having CNPAS, 27 patients had normal scans (control group), and 69 patients were excluded because of the presence of other craniofacial anomalies. All patients with CNPAS had evidence of abnormal fusion of the midline palatal suture. Zero patients without CNPAS had a midline palatal suture abnormality. The mean widths of the pyriform aperture were 5.7 mm (SD, 1.7) in the CNPAS group and 13.1 mm (SD, 2.7) in the control group (P < .0001). The mean distance between the superior portions of the nasolacrimal ducts was 9.1 mm (SD, 2.1) in the CNPAS group, and the mean of the control group was 13.4 mm (SD, 2.2) (P < .0001).
CONCLUSIONS: Patients with CNPAS have abnormal fusion of the midline palatal suture and exhibit lateral growth restriction of the midface. This may implicate synostosis of the midline palatal suture and abnormal midface growth.
ABBREVIATIONS:
- CNPAS
- congenital nasal pyriform aperture stenosis
- NLD
- nasolacrimal duct
Infants are obligate nasal breathers. As such, any degree of nasal airway obstruction may result in respiratory distress. Soft tissue edema caused by viral or idiopathic rhinitis is the most common cause of bilateral nasal obstruction in neonates. Less common, though clinically important, causes include choanal atresia and congenital nasal pyriform aperture stenosis (CNPAS).
CNPAS was first described in 1988 and 1989 in the radiology and otolaryngology literature, respectively.1,2 Since then, numerous case reports have highlighted 2 possible theories in the embryogenesis, as well as the presentation, diagnosis, and treatment.3⇓⇓⇓⇓-8 Historically, the 2 theories of embryogenesis are bony overgrowth of the nasal process of the maxilla and a primary deficiency of the hard palate, with most studies citing the former as the cause. Classically, symptoms include respiratory distress relieved by crying, difficulty feeding, nasal congestion, apnea, and failure to thrive. Physical examination may raise the suspicion for CNPAS when a 5F suction catheter cannot be passed through either nasal cavity; note that choanal atresia could have a similar finding. The diagnosis requires a maxillofacial CT revealing the pyriform aperture width to measure less than 11 mm.3,4 Associated imaging abnormalities include a median central incisor, a triangular-shaped palate, and a median palatal ridge. The presence of a median central incisor warrants further evaluation with MR imaging of the brain because it can occur as part of the holoprosencephaly spectrum.9 Genetic consultation may be useful to help define the presence of a syndrome. Treatment starts with medical therapy and, if needed, surgical therapy. Classically, surgical therapy involves drilling bone from the lateral extent of the pyriform aperture, though other entities such as dilation and rapid maxillary expansion have also been described.3⇓⇓⇓⇓⇓⇓⇓⇓⇓-13
As part of the primary author's previous work on CNPAS,11 a unique, never described radiographic feature was noted. The midline palatal suture appeared abnormally ossified and potentially fused, raising the possibility that CNPAS may be related to lateral growth restriction of the midface akin to craniosynostosis. Other studies have shown that narrowing of the nasal cavity extends posteriorly to include the middle and posterior portions of the nasal cavity, supporting this theory.3,14 With this in mind, we hypothesize that patients with CNPAS have abnormal midline palatal sutures and decreased midface dimensions compared with a control population.
MATERIALS AND METHODS
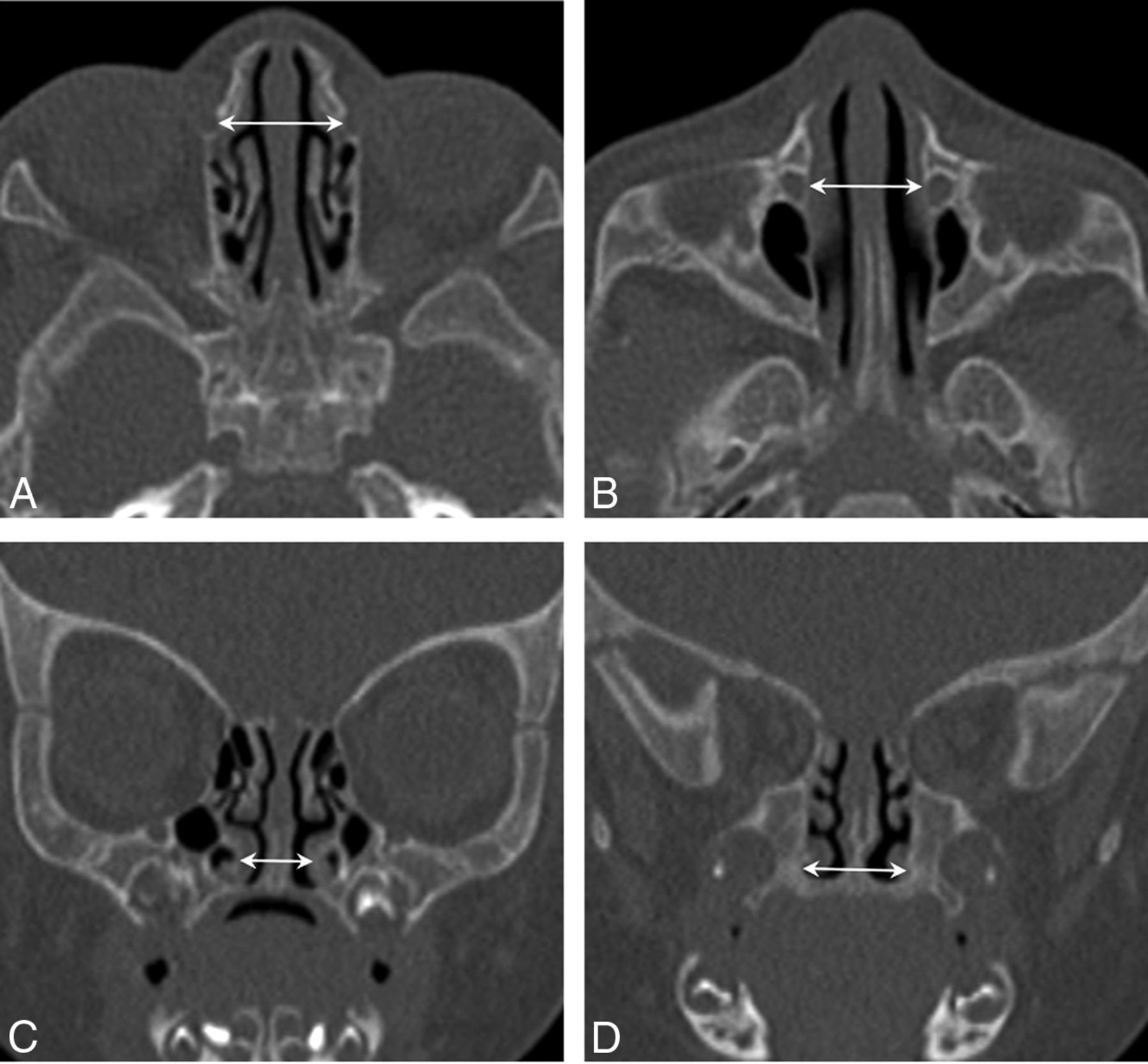
This single-center, retrospective study was approved by the local institutional review board of the University of Colorado and was compliant with the Health Insurance Portability and Accountability Act. Informed consent was waived. Pediatric patients aged 0 to 90 days who underwent maxillofacial CT between January 2003 and December 2013 were identified from our institution's electronic medical record data base. All scans were reviewed by a pediatric neuroradiologist (D.M.M.). Measurements of the width of the pyriform aperture were performed, with CNPAS defined as a pyriform aperture width less than 11 mm adhering to the original description of CT findings.3,4 Additionally, the width of the palate using the distance between the first molars, distance between the inferior turbinates, distance between the inferior aspects of the nasolacrimal ducts (NLDs), and distance between the superior aspects of the NLDs were acquired (Fig 1). Last, the midline palatal suture was evaluated for the presence or absence of ossification of the suture (Fig 2). Patients with additional craniofacial anomalies (eg, cleft lip and palate, Pierre Robin sequence, NLD cyst, and tumors of the head and neck) not associated with CNPAS were excluded. Gestational birth age, age at the time of CT, and other medical comorbidities were recorded. Descriptive statistics in each cohort were reported as median values (interquartile range [IQR]). The Mann-Whitney test was used to compare the 2 cohorts using P < .05 as the threshold allowing the null hypothesis to be rejected. The 95% CI between the medians of each cohort was computed using the Hodges-Lehmann estimate. Descriptive and comparative statistics were calculated using GraphPad Prism version 8.0.0 for Windows (GraphPad Software).

Normal midface measurements (arrows) of a control patient. A and B, Axial noncontrast CT images demonstrate normal widths between the superior and inferior aspects of the NLD, respectively. C, Coronal noncontrast CT image illustrates a normal width between the inferior nasal turbinates. D, Coronal noncontrast CT image shows a normal palatal width, which is measured at the level of the first molar.

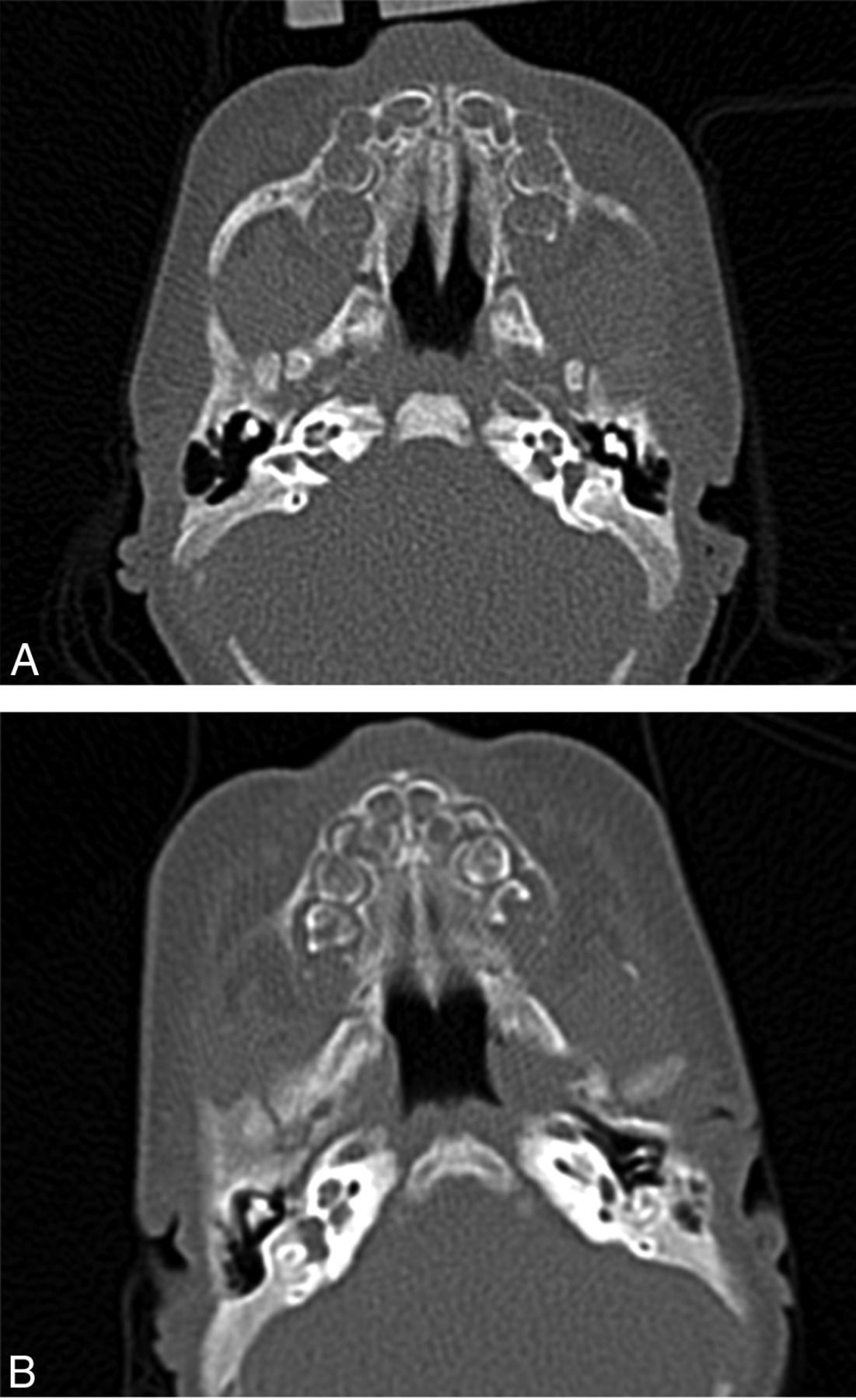
Midpalatal suture in control versus CNPAS. A, A normal midline palatal suture with no evidence of fusion. B, The midline palatal suture with midline ossification at the site of the suture.
RESULTS
A total of 109 patients aged 0–3 months underwent maxillofacial CT imaging at the Children's Hospital Colorado between January 2003 and December 2013. Thirteen patients had CNPAS, 27 had normal scans, and 69 had an additional craniofacial anomaly and were thus excluded from the study. The median gestational ages at birth were 38.0 (IQR, 35.0–40.0) weeks in the CNPAS and 40.0 (IQR, 38–40) weeks in the control group (P = .03). The ages at time of CT scan were 8.0 (IQR, 2.0–35.0) days in the CNPAS group and 15 (IQR, 5.0–47.0) days in the control group (P = .16). Fifty-four percent of patients were male.
The CNPAS cohort had a median pyriform aperture width of 6.0 (IQR, 4.8–7.6) mm compared with the control group measurement of 13.3 (IQR, 12.4–14.0) mm (P < .0001). The median width of the palate was 8.9 (IQR, 7.8–11.4) mm in the CNPAS group and 17.5 (IQR, 17.1–18.9) mm in the control group (P < .0001). The median distance between the inferior turbinates was 3.6 (IQR, 3.2–3.6) mm in the CNPAS group and 8.8 (IQR, 7.9–9.6) mm in the control group (P < .0001). The median distance between the inferior NLDs was 8.9 (IQR, 7.5–10.6) mm in the CNPAS group and 15.3 (IQR, 13.1–15.8) mm in the control group (P < .0001). The median distance between the superior NLDs was 9.3 (IQR, 7.8–11.3) mm in the CNPAS group and 13.6 (IQR, 12.7–14.5) mm in the control group (P < .0001). The difference between the medians and the 95% CI of difference for each measurement is listed in the Table. Thirteen of 13 patients in the CNPAS group had evidence of fusion of the midline palatal suture, of whom 11 had an associated midpalatal ridge (Fig 3). The midpalatal ridge actually appears as bony spinelike protrusion from the palate. Zero of 27 in the control group had a suture abnormality. Four of 13 patients with CNPAS had a median central incisor. Thirteen of 13 patients in the CNPAS cohort had nasal obstruction.

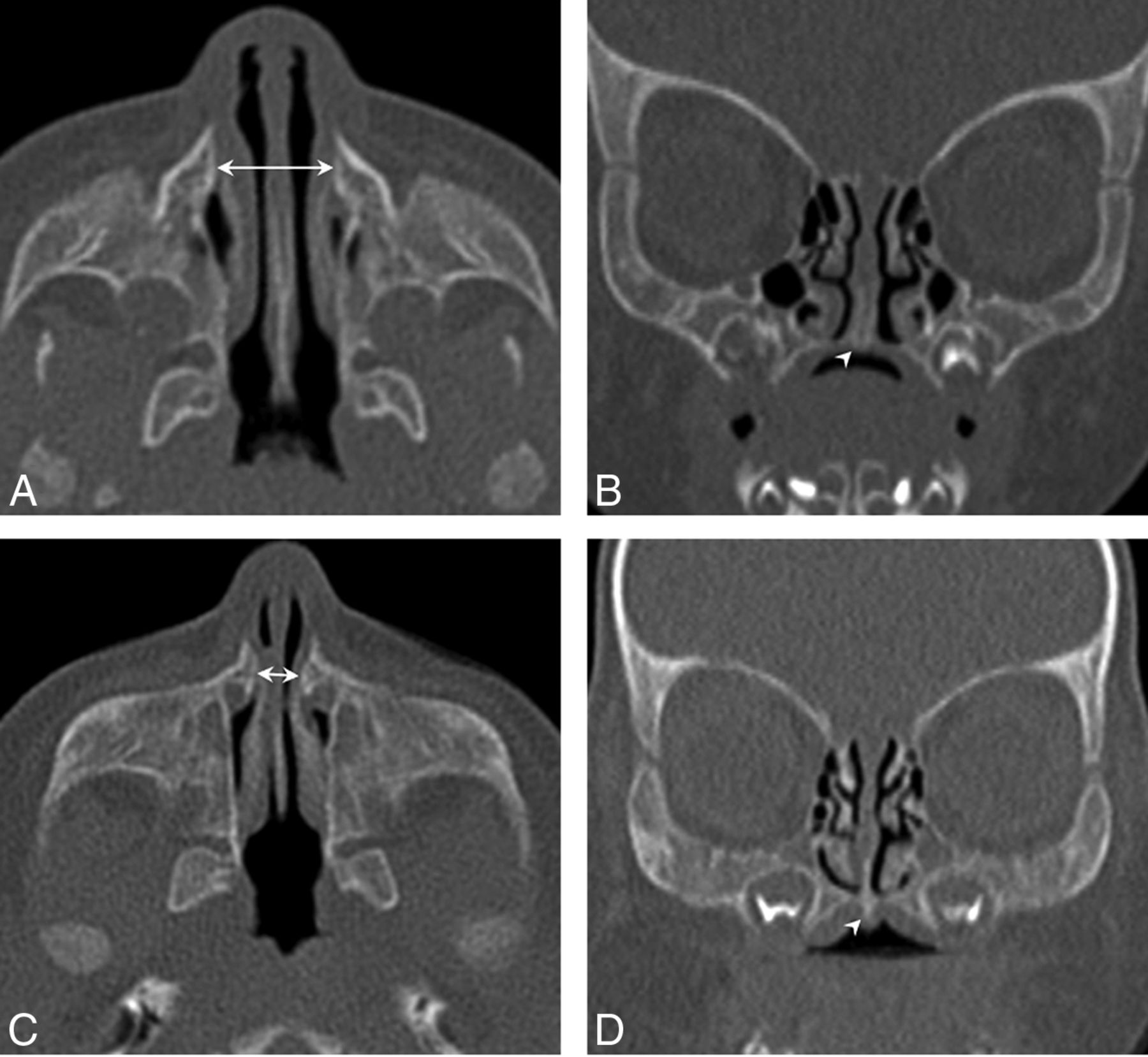
Normal and abnormal pyriform apertures and palates. A, Axial noncontrast CT image of a control patient where the arrow demonstrates normal pyriform aperture width. B, Coronal noncontrast CT image with arrowhead depicting absence of spinelike protrusion along the undersurface of the palate in the same control patient. C, Axial noncontrast CT image of a patient with CNPAS where the arrow depicts the abnormal narrowing of the pyriform aperture. D, Coronal noncontrast CT image with arrowhead depicting a spinelike protrusion along the undersurface of the reduced width palate in the same patient with CNPAS.
The difference in the median values of measured widths in CNPAS and control participants
DISCUSSION
The first clinical account of congenital nasal pyriform aperture stenosis (termed bony inlet stenosis) was in 1988.1 In this initial description, the authors proposed 2 theories of embryogenesis. The first was that excess ossification of the nasal process of the maxilla results in bony overgrowth and narrowing of the pyriform aperture. This theory is echoed throughout the literature.1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓-13 The second was that insufficient growth of the palate reduces the width of the pyriform aperture.
Many studies have demonstrated decreased width of the nasal cavity and palate in CNPAS. In our study, we also demonstrated that the midface was reduced in width by measuring the distance between the superior and inferior aspects of the NLDs. These findings provide evidence that CNPAS has deficient lateral growth of the midface to go along with the decreased width of the palate and the nasal cavity. With respect to the other developmental theory of CNPAS, excess ossification of the nasal process of the maxilla does not readily account for the reduced midface width between the inferior and superior aspects of the NLDs seen in our data.
Understanding the maturation process of the midline palatal suture has been clinically integral to understanding outcomes regarding rapid maxillary expansion.14 Although it is accepted that the midline palatal suture is open at birth, maturation and fusion start to happen in late adolescence.15 Knowing this, ossification of the midline palatal suture, seen in all 13 of our patients with CNPAS, is certainly intriguing. As a bony suture ossifies and closes, growth perpendicular to the long axis of the suture slows. If this occurs at the developmentally correct time, this occurs as the body is no longer growing. If this happens prematurely, as in the case of craniosynostosis, fusion of the cranial suture leads to growth restriction perpendicular to the suture. The features of CNPAS are similar. If the midline palatal suture matures prematurely, this could account for both the decreased horizontal palate growth and decreased midface growth, ultimately resulting in a restricted nasal cavity width consistent with CNPAS. Furthermore, this would explain the midline palatal ridge seen in most of our patients, similar to the type of ridging present in premature closure of the cranial sutures.
If growth restriction of the palate and midpalatal suture ossification occur in CNPAS, is overgrowth of the nasal maxillary process a cause of CNPAS as well? This study was not designed to discuss the presence of overgrowth of the nasal process of the maxilla in our CNPAS cohort. Thus, we are limited in our ability to compare the validity of 2 competing theories of CNPAS embryogenesis. It is possible that these 2 entities occur simultaneously as part of a developmental field defect as has been previously described,9,14 or it is possible that the relationship between them may be more akin to a sequence in which growth restriction causes an apparent overgrowth of the nasal maxillary process.
Another limitation of this study is that it is a single-center, retrospective review with a small cohort of patients. The study is further limited in that it was not intended to analyze clinical outcomes associated with these radiographic findings because the clinical outcomes of CNPAS are well described.
The importance of this study is that it highlights abnormal ossification of the midline palatal suture and decreased midfacial dimensions in CNPAS. This can clarify the etiology and can lead to further study involving the origin and treatment of CNPAS. Although we are unable to prove causality, it is quite plausible that CNPAS is secondary to premature ossification of the midline palatal suture, which we term “palatal synostosis.” If CNPAS is the result of palatal synostosis, like craniosynostosis, early surgical intervention to the prematurely fused suture could provide consideration for new therapeutic options.
CONCLUSIONS
Congenital nasal pyriform aperture stenosis has reduction of midface growth. Premature ossification of the midline palatal suture, palatal synostosis, may be central to the development of CNPAS. Further experience following these patients may allow more understanding into the long-term growth characteristics of the midface in patients with CNPAS.
Footnotes
Data previously presented at: American Society of Pediatric Otolaryngology Spring Meeting, May 2015; Boston, Massachusetts.
Disclosures: Jeremy Prager—UNRELATED: Board Membership: EvoEndo Inc, Comments: Board member, medical device company focused on endoscopy*; Patents (Planned, Pending or Issued): EvoEndo Inc, Comments: Several patents issued*; Stock/Stock Options: EvoEndo Inc.*, Comments: Founders stock. *Money paid to the individual author.
References
- Received July 1, 2020.
- Accepted after revision December 22, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.