
Abstract
BACKGROUND AND PURPOSE: Second opinion reports of neurologic head and neck imaging are requested with increased regularity, and they may contain a recommendation to the clinician. Our aim was to investigate the frequency and determinants of the presence of a recommendation and the adherence by the referring physician to the recommendation in a second opinion neurology head and neck imaging report and the diagnostic yield of these recommendations.
MATERIALS AND METHODS: This retrospective study included 994 consecutive second opinion reports of neurology head and neck imaging examinations performed at a tertiary care center.
RESULTS: Of the 994 second opinion reports, 12.2% (121/994) contained a recommendation. An oncologic imaging indication was significantly (P = .030) associated with a lower chance of a recommendation in the second opinion report (OR = .67; 95% CI, 0.46–0.96). Clinicians followed 65.7% (88/134) of the recommendations. None of the investigated variables (patient age, sex, hospitalization status, indication for the second opinion report, experience of the radiologist who signed the second opinion report, strength of the recommendation, and whether the recommendation was made due to apparent quality issues of the original examination) were significantly associated with the compliance of the referring physician to this recommendation. The 134 individual recommendations eventually led to the establishment of 52 (38.2%) benign diagnoses and 28 (20.6%) malignant diagnoses, while no definitive diagnosis could be established in 56 (41.2%) cases.
CONCLUSIONS: Recommendations are relatively common in second opinion reports of neurology head and neck imaging examinations, though less for oncologic indications. They are mostly followed by requesting physicians, thus affecting patient management. In most cases, they also lead to the establishment of a diagnosis, hence adding value to patient care.
ABBREVIATION:
- NHN
- neurology head and neck
Tertiary care radiology departments frequently review imaging examinations that have been performed and interpreted elsewhere.1,2 Neurology head and neck (NHN) imaging examinations comprise a large proportion of second opinion reports that are generated at tertiary care centers.2
At present, there is an increase in the overall number of second opinion readings.1 This also applies to second opinion re-evaluations of NHN imaging examinations, with reported growth rates of 245% in the United States from 2011 to 2015.3 Many hospitals also require an official record in the form of a second opinion report to be provided for all outside studies, which may also take extra time. This policy is followed by 37.4%–60.0% of the radiology departments in the United States.4 Altogether, the workload of radiologists due to second opinion interpretations is increasing.
Second opinion interpretations may potentially be beneficial to patient care by avoiding unnecessary additional imaging examinations, improving disease detection, and establishing a more accurate differential diagnosis.2,5⇓⇓⇓-9 Tertiary care radiologists may also give a recommendation in the second opinion report to provide guidance on patient management to the clinician. These recommendations may include advice to perform additional imaging, perform a biopsy, refer the patient to another specialty, or compare an examination with previous imaging examinations, among others.
Currently, it is unclear how many second opinion reports of NHN imaging examinations contain a recommendation to the clinician, which factors are associated with the presence of a recommendation in the second opinion report, how frequently the recommendation is followed by the clinician, and which factors affect the adherence of the clinician to the recommendation. Such information would be valuable to determine whether the practice of second opinion reporting with the provision of a recommendation to the clinician affects patient management in the field of NHN imaging. In addition, it is unknown how many of these recommendations eventually allow the establishment of a diagnosis. This information is important to understand their contribution to value-based patient care.
The purpose of this study was, therefore, to investigate the frequency and determinants of the presence of a recommendation and the adherence by the referring physician to the recommendation in a second opinion NHN imaging report and the diagnostic yield of these recommendations.
MATERIALS AND METHODS
Study Design
The local institutional review board of the University Medical Center Groningen approved this retrospective single-center study, and informed consent was waived. All consecutive second opinion reports of NHN imaging examinations that were compiled in our tertiary care center in the Netherlands within a 1-year time period (November 2016 to November 2017) were potentially eligible for inclusion in this study. A second opinion report was included if the original imaging examination was performed and reported in another hospital before referral to our center. A second opinion report was excluded if its content mentioned that no re-evaluation was performed because the second opinion reading became clinically irrelevant due to the availability of more recent imaging examinations, if either the report or the imaging examination was not available in the hospital’s PACS, if the re-evaluated imaging examination did not primarily concern NHN imaging (eg, CT of neck, chest, and abdomen in a patient with lymphoma), or if it concerned a re-evaluation of an in-house imaging examination.
Local Practice of Second Opinion Readings
In our department, an outside imaging examination is only reviewed if the treating clinician contacts one of the radiologists and obtains his or her approval for the second opinion reading. The decision to accept or reject the second opinion request is based on the conversation between the clinician and radiologist, and not by a review of the images beforehand. The radiologist accepts all second opinion readings of patients who will be discussed in a multidisciplinary meeting. If patients will not be discussed in a multidisciplinary meeting and the tertiary care radiologist does not see any advantage to re-evaluate a scan that was already interpreted by another radiologist elsewhere (eg, if a case concerns common pathology that is also frequently seen by radiologists who work in nonacademic hospitals), the second opinion request is rejected. The imaging examination and the primary report that was composed in the hospital from which the patient was referred need to be uploaded to our PACS. After review of the relevant imaging examinations, an official written second opinion report is then compiled and made available to the referring physician in the hospital’s electronic patient file system. Radiologists (regardless of years of experience) are authorized to report and sign second opinion reports. There is a rule in our department to refrain from any curbside consultations to maintain quality. Note that at the time that our study was performed, the Dutch Healthcare Authority had a rule in place that it was not possible to submit second opinion readings for billing when patients were referred from one hospital to a treating physician in another hospital.
Data Extraction
For each second opinion report, we collected the following variables: patient age, sex, hospitalization status (in- or outpatient) at the time of the second opinion reporting, imaging indication (developmental, infectious, inflammatory, neurodegenerative, oncologic, benign sellar/parasellar tumors, trauma, vascular, miscellaneous), imaging technique (CT, MR imaging, ultrasonography, or x-ray), years of experience of the radiologist who signed the second opinion report (calculated from the end of residency), whether this radiologist was subspecialized in NHN imaging, and the presence of a recommendation in the second opinion report. Recommendations made in the second opinion report were evaluated as follows: type of recommendation (recommendation for additional imaging, biopsy, referral to another specialty, comparison with previous imaging examinations, or other), strength of the recommendation (hard [eg, wording such as“ it is advised to” or “it is indicated to”] or soft [eg, “it can be considered to” or “suggest”]) based on a predefined categorization scheme applied by 2 independent raters (S.A.H. and T.C.K., who were blinded to each other’s ratings), whether the recommendation was made due to apparent quality issues of the original imaging examination (ie, insufficient diagnostic quality, including missing sequences for MR imaging), compliance of the referring clinician to the recommendation, and the diagnostic outcome related to the recommendation.
For second opinion reports with a recommendation, the diagnosis in the primary report was compared with the diagnosis in the second opinion report. Referring clinicians’ compliance to the recommendation in the second opinion report was determined on the basis of the records in the hospital’s electronic patient file system—ie, if the recommended procedure was performed after the second opinion report had been authorized and if there was a clear connection to the recommendation, it was considered to have been followed. The diagnostic outcome of a recommendation was determined on the basis of all available follow-up data during a minimum 2-year follow-up, using 3 categories: A benign diagnosis was established, a malignant diagnosis was established, or no diagnosis could be established even though additional diagnostic procedures may have been performed. Note that our country has a well-developed infrastructure to exchange patient data among hospitals, which allowed tracing follow-up studies outside our hospital if they were performed.
Statistical Analysis
The frequency of second opinion reports with a recommendation as a proportion of the total number of second opinion reports was calculated. The Cohen κ was run to determine the interrater agreement regarding the strength of the recommendations. Logistic regression analyses were performed to determine the association of the presence of a recommendation in the second opinion report with the following variables: patient age, sex, hospitalization status, indication for the second opinion report, and experience and NHN subspecialization of the radiologist who signed the second opinion report.
The frequency of the referring clinicians’ compliance to the recommendations in the second opinion reports was also calculated. Logistic regression analyses were performed to determine the association of the referring clinicians’ adherence to the recommendation in the second opinion report with the following variables: patient age, sex, hospitalization status, indication for the second opinion report, experience and NHN subspecialization of the radiologist who signed the second opinion report, the strength of the recommendation, and whether the recommendation was made due to apparent quality issues of the original examination.
P values < .05 were deemed statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, Version 23; IBM).
RESULTS
Second Opinion Reports
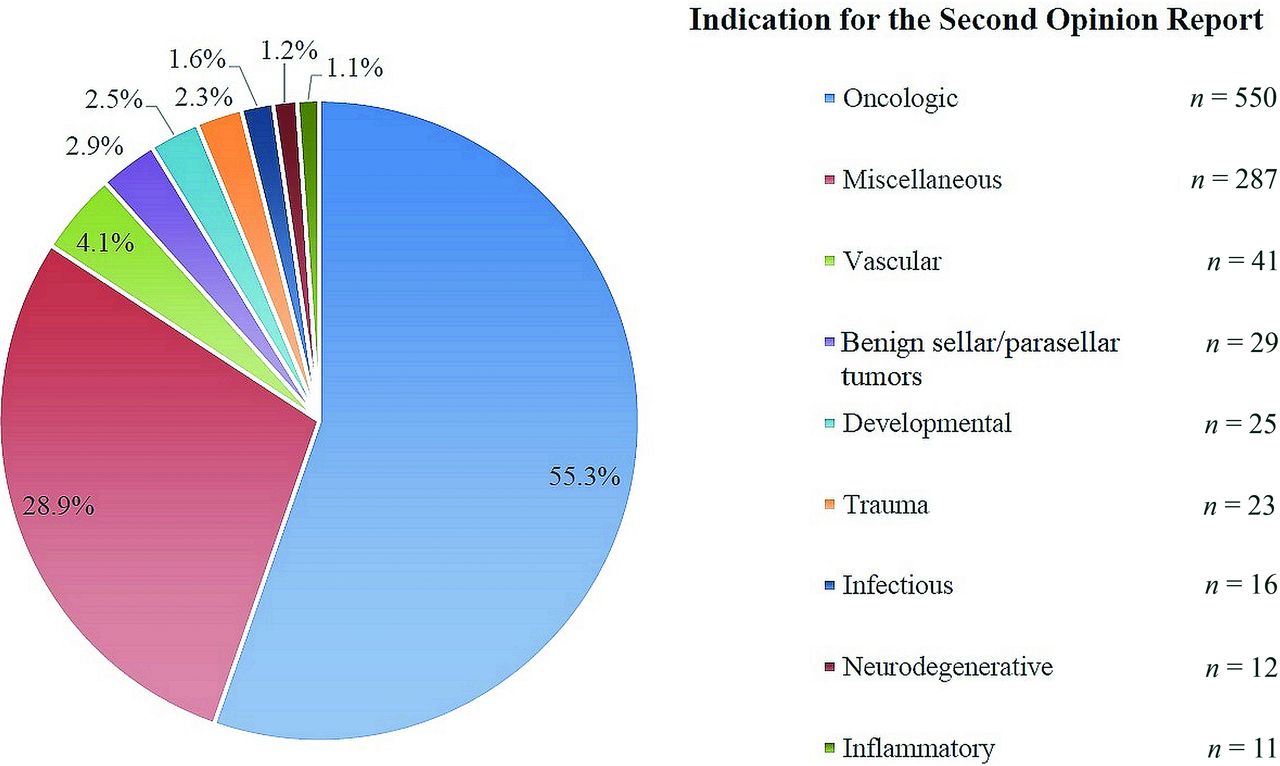
A total of 1038 second opinion reports of NHN imaging examinations were made at our tertiary care center between November 2016 and November 2017. Of these 1038 second opinion reports, 22 were excluded because no re-evaluation was performed because the second opinion reading became clinically irrelevant due to the availability of more recent imaging examinations, 11 were excluded because the report or the imaging examination was not available in the hospital’s PACS, 10 were excluded because they did not primarily concern NHN imaging, and 1 was excluded because it concerned a re-evaluation of an in-house imaging examination. Eventually, 994 second opinion NHN imaging examinations were included, of which 115 (11.6%) involved comparisons with previous second opinion readings. These 994 second opinion reports concerned 453 male and 541 female patients, with a mean age of 50 (SD, 24) years (range, 0–96 years). Most patients were outpatients (92.4%), most imaging examinations were performed for oncologic reasons (55.3%), almost all imaging examinations concerned MR imaging (79.5%) or CT (19.8%), and most of the second opinion reports comprised 1 imaging examination (86.9%) (Table 1 and Figure). The second opinion reports were authorized by 20 radiologists, of whom 8 were subspecialized NHN radiologists. The mean number of second opinion reports per radiologist was 49.7 (SD, 65.1) (range, 1–197). The mean experience of the radiologists was 12 (SD, 9) years after completion of residency (range, 0–29 years).

Frequencies of the different imaging indications for the 994 second opinion reports included in this study.
Patient and NHN examination characteristics for which a second opinion report was requested (n = 994)
Recommendations in Second Opinion Reports and Determinants
Of the 994 second opinion reports, 12.2% (121/994) contained a recommendation. The number of individual recommendations totaled 134, because there were 112 reports with a single recommendation, 8 with 2 recommendations, and 2 reports with 3 recommendations. Apparent quality issues of the original imaging examination were responsible for 14.2% (19/134) of recommendations (Table 2). Recommendations involved additional imaging in 82.8% (111/134) and nonimaging procedures in 17.2% (23/134) (Table 3). The same examination (same technique, same body region) as the original study was recommended in 50 cases, of which 8 issues were due to the quality of the original imaging examination. Interrater reliability regarding the strength of the recommendation was almost perfect with κ = 0.954 (95% CI, 0.924–0.984). Most recommendations (48.5%) were issued by radiologists with 6–15 years of experience after residency (Table 4). Univariate logistic regression showed that an oncologic imaging indication was significantly (P = .030) associated with a lower chance of a recommendation in the second opinion report (OR = 0.67; 95% CI, 0.46-0.96). There were no significant associations between the presence of a recommendation in the second opinion report and any other of the variables that were investigated. Therefore, no further multivariate analysis was performed.
Specifications of the 134 recommendations made in 121 of 994 NHN second opinion reportsa
Distribution of recommendations according to 5 groups for recommendations that were followed, that were not followed, and for which it remained unclear whether the recommendation was followed (n = 134)
Distribution of categorized experience of the radiologist for recommendations that were followed, that were not followed, and for which it remained unclear whether the recommendation was followed (n = 134)
Clinicians’ Compliance to Recommendations in Second Opinion Reports and Determinants
Clinicians followed 65.7% (88/134) of the recommendations (Table 3). Medical follow-up records of at least 2 years confirmed that we did not miss any diagnostic test or other action performed at an outside/remote facility that was related to the recommendation in the second opinion report (ie, the treating physician in our academic hospital kept track of these patients and updated their medical documentation for a minimum of 2 years, as evidenced by our review of the medical records). Most interesting, 50% (44/88) of the recommendations that were followed were issued by radiologists with 6–15 years of experience after residency (Table 4). Note that for 4 recommendations, it remained unclear whether they were followed. Because 127 of the remaining 130 recommendations were issued by NHN radiologists, no meaningful statistical analysis could be made on the association between the referring clinicians’ compliance with a recommendation in the second opinion report and the subspecialty of the radiologist (NHN versus other) who signed the second opinion report. Otherwise, there were no significant associations between the referring clinicians’ compliance with the recommendation in the second opinion report and any of the variables that were investigated.
Diagnostic Outcome Related to Recommendations in Second Opinion Reports
For second opinion reports with a recommendation, the diagnosis in the primary report was different from that in the second opinion report in 43 (35.5%) of 121 cases. No diagnostic change was found in 68 (56.2%) cases, whereas in the remaining 10 (8.3%) cases, the primary report was either unavailable or the second opinion report referred to only the poor quality of the imaging examination without mentioning a diagnosis. A definitive diagnosis could be established for 80 (59.7%) recommendations. This was based on additional procedures and test results in 69 (86.3%) cases and in 11 (13.8%) cases on the imaging examination for which the second opinion reading was requested. In total, the 134 individual recommendations in the second opinion reports eventually led to the establishment of 52 (38.2%) benign diagnoses and 28 (20.6%) malignant diagnoses, while no definitive diagnosis could be established in 56 (41.2%) cases (Table 5). Most benign diagnoses were established on the basis of imaging examinations (n = 31, 59.6%); most malignant diagnoses were based on biopsies (n = 15, 53.6%) (Table 6). Note that 2 second opinion reports, each with a single recommendation, both led to 2 different diagnoses, as a result of which the total number of established and unestablished diagnoses was 136.
Distribution of diagnostic outcome for recommendations that were followed, that were not followed, and for which it remained unclear whether the recommendation was followed (n = 136)a
Reference standards of the established benign and malignant diagnoses in the study sample (n = 80)
DISCUSSION
The results of this study show that 12.2% of second opinion reports of NHN imaging examinations contain a recommendation and that this recommendation was followed by the referring physician in 65.7% of cases. In addition, the recommendations that were made in the second opinion report led to a definitive diagnosis (either benign or malignant) in most cases. Also of interest is that for second opinion reports with a recommendation, the diagnosis of the primary report had already changed with the second opinion reading itself in about one-third of cases. These data indicate that the practice of second opinion reporting in NHN imaging, with a provision of a recommendation to the clinician when appropriate, adds clinical value. They also support that the increasing workload of academic radiologists due to the continuing increase in requests for second opinion reports of NHN imaging examinations1,3 should be acknowledged by health care systems, insurance companies, and policy makers. Of note, at present, neither our department nor our hospital receives any reimbursement for the second opinion readings that are performed.
Our results also show that second opinion reports of imaging examinations with an oncologic indication had an approximately one-third lower chance of containing a recommendation than those with other imaging indications. This is probably because for many common NHN cancers (eg, cerebral glioma or head and neck squamous cell carcinoma), differential diagnostic dilemmas are less common and the subsequent diagnostic work-up is protocolized and well-known among both radiologists and referring physicians.10⇓⇓–13 The finding that radiologists relatively less frequently add a recommendation to their second opinion report in these circumstances may be potentially useful when weighing the expected benefits against the labor spent on a second opinion report when clinicians submit a second opinion request.
On the other hand, none of the patient and second opinion variables that were investigated were significantly associated with the referring physician’s adherence to the recommendation in the second opinion report. Of interest, a previous study by our research group showed that 16.4% (191/1,163) of second opinion NHN imaging reports in our patient population in 2018 were actually never read at all by a clinician.14 In that same study that included second opinion reports from all different radiologic subspecialties, it was also reported that second opinion reports with neurology as the requesting specialty were significantly (P < .001) more prone to remaining unread compared with other requesting specialties (including otorhinolaryngologists) (OR = 2.82; 95% CI, 1.78–4.47).14 Why neurologists more frequently refrain from reading the second opinion report they request remains unclear, but it explains why some recommendations were not followed. Of note, the present study was performed between November 2016 and November 2017, when it was not yet possible to verify whether second opinion reports were read due to technical limitations. However, because the clinical scenario in our previous study14 is the same as in the present study, the “nonreading” percentage of 16.4% is probably also applicable to the current data set. Further research is necessary to identify other sources of noncompliance to the recommendation in the second opinion report.
There is ample literature on the frequency of recommendations for additional imaging and the adherence by clinicians to these recommendations when it comes to primary imaging readings. For example, a study by Sistrom et al15 analyzed 5,948,342 radiology reports of different modalities performed between 1995 and 2008 and reported that recommendations for additional imaging increased during the 13 years of the study, with the unadjusted rate rising from roughly 6% to 12%. In another more recent study by Mabotuwana et al16 that analyzed 2,972,164 radiology examinations performed between 2010 and 2017, there was at least 1 recommendation for follow-up imaging in 10.6% of radiology reports, while the overall follow-up imaging adherence rate was 58.1%. However, the studies by Sistrom et al15 and Mabotuwana et al16 did not concern second opinion reports, did not focus on NHN imaging, and did not consider recommendations for nonimaging procedures. Nevertheless, the frequencies of recommendations and compliance rates are quite similar between the present study and those reported by Sistrom et al15 and Mabotuwana et al.16
Literature on the topic of second opinion readings is scarce. A previous study by Heinz et al17 analyzed 2225 second opinion reports of abdominal imaging examinations performed at outside institutions. They reported that 10.4% of secondary abdominal imaging interpretations contained a recommendation for additional imaging and that patient age and the experience of the radiologist who performed the secondary interpretation were independently significantly associated with the presence of a recommendation for additional imaging.17 Heinz et al18 also reported an adherence rate of 53.1% to recommendations in second opinion radiology reports of abdominal imaging examinations, while no determinants of the referring physician’s compliance could be identified. Finally, the recommendations that were made in the second opinion reports in the study by Heinz et al18 led to a definitive diagnosis in 41.1%. Although this previous work by Heinz et al17,18 was performed in the setting of abdominal imaging, their results on the frequency of recommendations, compliance rate, and diagnostic yield largely resonate with the findings of the present study. A study by Torok et al19 included 11,753 reports of their Neuroradiology Second Opinion Consultation Services to analyze requests for repeat imaging. In their study, repeat imaging studies were recommended in 1.5% of cases.19 In addition, in 0.3% of all cases, a subsequent repeat examination was documented in the electronic medical records.19 However, the study of Torok et al19 was focused only on recommendations for repeat imaging, used a search strategy based on keywords, and may have underestimated the rate of followed recommendations due to missing clinical information.
The present study had several limitations. First, this study was performed at a tertiary care center where all medical specialists receive a fixed salary, regardless of the number of procedures performed. Therefore, there were no financial incentives for radiologists to add a recommendation to the second opinion report or for referring physicians to follow a recommendation. However, it is unclear whether the results of our study are also applicable to institutions in which the remuneration of medical specialists is, in part, dependent on production numbers.16,20,21 Second, most second opinion reports concerned oncologic patients. It is unclear whether the results of this study are generalizable to institutions that provide health care services to a different spectrum of patients undergoing NHN imaging. Third, most recommendations were made by NHN radiologists. Therefore, no logistic regression analysis could be made to compare the compliance of referring physicians with the recommendations made by NHN radiologists versus other radiologists, and no subgroup analyses could be performed to compare these 2 groups in terms of diagnostic yield related to the recommendations made. Thus, it remains unclear if recommendations in second opinion NHN imaging reports made by radiologists without NHN subspecialization also affect patient care. Fourth, there was no analysis on whether the recommendations in the second opinion reports actually improved patient outcome. Fifth, the diagnostic outcome was not always established on the basis of additional procedures and diagnostic tests, but on the imaging examination for which a second opinion reading was requested. This issue may limit the reliability of the established diagnoses. Sixth, because virtually all conversations between clinicians and radiologists about second opinion requests take place on nonrecorded phone calls, it remains unclear how many second opinion requests were rejected.
CONCLUSIONS
Recommendations are relatively common in second opinion reports of NHN imaging examinations, though this is less the case for oncologic indications. They are mostly followed by requesting physicians, thus affecting patient management. In most cases, they also lead to the establishment of a diagnosis, hence adding value to patient care.
References
- Received December 16, 2020.
- Accepted after revision April 5, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.