
Abstract
BACKGROUND AND PURPOSE: The traditional Papile classification system for severe germinal matrix hemorrhage–intraventricular hemorrhage is limited in objectivity and interrater variability for accurate prediction of neurodevelopmental impairment in extremely preterm infants. Many extremely preterm infants with severe germinal matrix hemorrhage–intraventricular hemorrhage are still offered “redirection of care” in spite of the recent evidence suggesting that many of these infants can have normal outcomes. Therefore, it is important to consider the laterality and extent of brain hemisphere involvement while classifying severe germinal matrix hemorrhage–intraventricular hemorrhage to predict neurodevelopmental impairment. The aim of the present study was to compare the Al-Abdi system with the Papile system for their accuracy in predicting neurodevelopmental impairment in extremely preterm infants with severe germinal matrix hemorrhage–intraventricular hemorrhage.
MATERIALS AND METHODS: This is a retrospective study of extremely preterm infants with severe germinal matrix hemorrhage–intraventricular hemorrhage admitted to a tertiary neonatal intensive care unit (2006–2016). Cranial sonograms were independently re-reviewed by 2 radiologists as per the Al-Abdi system. The prognostic statistical indices for both systems to predict neurodevelopmental impairment were calculated.
RESULTS: A total of 91 infants with severe germinal matrix hemorrhage–intraventricular hemorrhage survived, and 83 (median gestational age, 26.3 weeks; and median birth weight, 890 g) completed developmental assessment. The receiver operating characteristic areas under the curve to predict neurodevelopmental impairment by the Papile versus Al-Abdi systems were 0.702 versus 0.723, respectively (P = .474). Corresponding Al-Abdi cutoff scores of 19, 20, 21, and 22 demonstrated increased specificity (76.36%–85.45%) and correct classification (69.88%–72.29%) to predict moderate-to-severe neurodevelopmental impairment.
CONCLUSIONS: The Al-Abdi system is comparable with the Papile system for predicting neurodevelopmental impairment for extremely preterm infants with severe germinal matrix hemorrhage–intraventricular hemorrhage, with higher Al-Abdi scores being more specific. This finding may prove useful for neonatal health care providers and parents in their decision regarding “continuation of care.” Future multicentric studies are warranted to ascertain the validity of individual Al-Abdi scores.
ABBREVIATIONS:
- AUC
- area under the curve
- BSID
- Bayley Scales of Infant and Toddler Development
- BW
- birth weight
- CP
- cerebral palsy
- EP
- extremely preterm
- GA
- gestational age
- GMDS
- Griffiths Mental Developmental Scale
- GMFCS
- Gross Motor Functional Classification System
- GMH–IVH
- germinal matrix hemorrhage–intraventricular hemorrhage
- NDI
- neurodevelopmental impairment
- NICU
- neonatal intensive care unit
- PVHI
- periventricular hemorrhagic infarction
- ROC
- receiver operating characteristic
Improved survival of extremely preterm (EP) infants, consequent to recent advances in obstetric and neonatal care, has shifted the focus on morbidities associated with neurodevelopmental impairment (NDI).1⇓⇓⇓-5
Germinal matrix hemorrhage–intraventricular hemorrhage (GMH-IVH) is one such morbidity, which has largely remained unchanged across time, with an estimated prevalence rate of 20%–30% in this high-risk group.6,7 Papile et al8 had classified grades of GMH-IVH from 1 to 4. Grade 1 includes hemorrhage confined to the subependymal germinal matrix; grade 2 includes hemorrhage into the lateral ventricles without ventricular dilation; grade 3 involves GMH-IVH with ventricular dilation; and grade 4 includes GMH-IVH with parenchymal involvement.8 Traditionally, severe (grades 3 and 4) GMH-IVH is considered a major determinant of poor neurodevelopmental outcome. Currently, the Papile system remains the most commonly used method for classification of GMH-IVH and prognostication based on the grade. However, there are a few concerns about using this traditional method of classifying GMH-IVH because of a lack of objectivity in reporting higher grades of GMH-IVH and a high interrater variability. Furthermore, recent literature indicates that preterm infants with grade 4 GMH-IVH or parenchymal bleed have a relatively better long-term prognosis than previously thought.9 Hence it becomes important to take into consideration the laterality and extent of brain hemisphere involvement with GMH-IVH to predict long-term neurodevelopment and to support any clinical decision regarding redirection or escalation of care of these EP infants.10⇓-12
The novel reporting system of GMH-IVH based on laterality (unilateral versus bilateral) was developed by Al-Abdi13 to try to overcome the shortcomings of the older Papile classification system. This objective system can reclassify the broader grades 3 and 4 GMH-IVH of the existing Papile system into different scores. The neurodevelopmental outcomes can then be predicted for each individual score, helping in better outcome-prediction models and possibly proving immensely helpful in the decision regarding the “redirection” or “continuation of care” for these EP infants with severe GMH-IVH. However, there is a dearth of data to establish the usefulness of this new classification system. A recent study of 183 preterm infants by Al-Mouqdad et al14 found that the newer classification system by Al-Abdi had more enhanced specificity to predict NDI than the traditional Papile classification system.
The objective of our study was to compare the ability of the newer GMH-IVH Al-Abdi classification system to predict the NDI compared with the older classification system by Papile et al.8
MATERIALS AND METHODS
Design and Setting
This was a retrospective study in the sole tertiary referral neonatal intensive care unit (NICU) in Western Australia.
Ethics Approval
Approval from the institutional Governance Evidence Knowledge Outcomes committee (project approval number: 33531) was obtained before commencing the study.
Eligibility
All preterm infants born before 28 weeks’ gestation (EP infants) and admitted to the NICU between January 2006 and December 2016 were eligible. Serial screening cranial ultrasounds are performed on days 1, 7, and 28 for all preterm infants of <33 weeks’ gestational age (GA) as routine practice in our NICU. For the purpose of our study, we included only those infants with GMH-IVH classified as severe (grade 3 or 4) as per the classification system of Papile et al.8
Exclusion
EP infants with congenital or chromosomal anomalies and outborn infants were excluded from the study. We also excluded EP infants who died during the hospital stay or were lost to follow-up because their neurodevelopmental outcomes were not available.
Data Collection
Neonatal demographic and clinical data until the time of death or discharge from NICU were extracted from the neonatal electronic data base. Maternal demographic and risk factors (eg, pre-eclampsia, prolonged rupture of membranes, chorioamnionitis, and antenatal glucocorticoids) were recorded. Neurodevelopmental scores up to 36 months’ corrected age were collected from our institutional Neonatal Follow-Up Program data base. The final outcome of NDI was considered the criterion standard in assessing the performance of the Al-Abdi versus Papile systems for their diagnostic utility.
Cranial Sonography Details
Cranial sonography was performed by an experienced sonographer using an Acuson S2000 sonography system (Siemens) equipped with a multifrequency sector transducer (4–10 MHz). Sonography was performed in the coronal and sagittal/parasagittal planes through an anterior fontanelle, obtaining sequential images. The images were stored digitally on the IMPAX electronic data base (https://www.impaxcorp.com/) and subsequently reported by experienced senior radiologists. A repeat assessment of the cranial sonography images was independently performed by 2 expert radiologists (S.M. and W.T.) for scoring per the Al-Abdi system.
Al-Abdi Scoring System
The Al-Abdi system involves squaring of the highest traditional GMH-IVH grade (GMH-IVH grades 1, 2, 3, 4 as per the Papile classification with corresponding Al-Abdi scores of 1, 4, 9, or 16, respectively), plus the GMH-IVH grade on the contralateral side, plus 5 for each hemisphere when >2 of its territories are involved, and plus 5 when there is a midline shift of the brain. “Territories” refer to the brain regions from the system of Bassan et al.10 The scores can have a maximum value of 35 (42 plus 4 plus 5 plus 5 plus 5) for a bilateral grade 4 GMH-IVH with a midline shift and involving >2 territories in either of the hemispheres (Fig 1).13 The 2 radiologists involved in the study were completely blinded to the final neurodevelopmental outcomes of the included preterm infants.

Al-Abdi score image. LOGIQ E9 indicates ultrasound machine that was used to capture the image.
Neurodevelopmental Assessments
The neonatal follow-up program at King Edward Memorial Hospital for Women and Newborn (Subiaco, Western Australia) institution is offered to all infants born at <28 weeks’ GA or <1000-g birth weight (BW) for standardized developmental, growth, and medical assessment at 12 , 24, and 36 months and 5 years of age.
Measures
The Griffiths Mental Developmental Scale (GMDS 0–2 years and the GMDS-Extended Revised/ER 2–8 years)15 were offered at 12 and 36 months’ corrected age, and the Bayley Scales of Infant and Toddler Development (BSID, 2nd and 3rd editions),16,17 at 24 months’ corrected age. Each measure comprises standard psychometric properties based on published norms, with a mean of 100 and an SD of 15, with the exception of the GMDS, which has a mean of 100 and an SD of 12. Cognitive scores from the BSID and the developmental quotient from the Griffiths assessments were used in this analysis. The GMDS and GMDS-Extended Revised were administered by accredited neonatal pediatricians, and the BSID was administered by registered psychologists. The most recent quotient score was analyzed for each child because this has been shown to correlate well with long-term outcomes.18
Definitions
Cerebral palsy (CP) was defined clinically as a nonprogressive disorder of movement and posture in the presence of tone abnormalities, and when possible, it was classified under the Gross Motor Functional Classification System (GMFCS). CP status was verified against the West Australian Register of Developmental Anomalies–Cerebral Palsy register.
Mild impairment was defined as a cognitive score >1–2 SDs below the test mean, ambulant CP (GMFCS level I/II), and unilateral deafness. Moderate impairment was defined as cognitive scores >2–3 SDs below the mean, GMFCS level III CP (ambulant with aids), and bilateral deafness needing amplification. Severe impairment was defined as cognitive scores of >3 SDs below the mean, GMFCS level IV/V CP, and blindness (vision, <6/60). Autism was not specifically assessed but was classified as a severe outcome if known to be present and diagnosed by standard multidisciplinary team assessment.19 The maternal socioeconomic status was measured using the Socio-Economic Indexes for Areas of relative advantage-disadvantage statewide decile data based on postcodes at birth (Australian Bureau of Statistics).
Data Analysis
Continuous data were summarized using median, interquartile range, and range and categoric data, using frequency distributions. The statistical indices, sensitivity, specificity, receiver operating characteristic curve (ROC), and area under the curve (AUC) for the Papile and the Al-Abdi scores to predict NDI were calculated using STATA, Version 16 statistical software (StataCorp). Furthermore, the diagnostic utility of the Papile grading and Al-Abdi scores for the prediction of moderate-to-severe NDI was assessed using predicted probabilities from separate logistic regression models, including GA, BW z score, oxygen at 36 weeks, and socioeconomic status (lowest 2 quintiles) in the ROC analysis; and the AUC was compared between systems. P values < .05 were considered statistically significant.
RESULTS
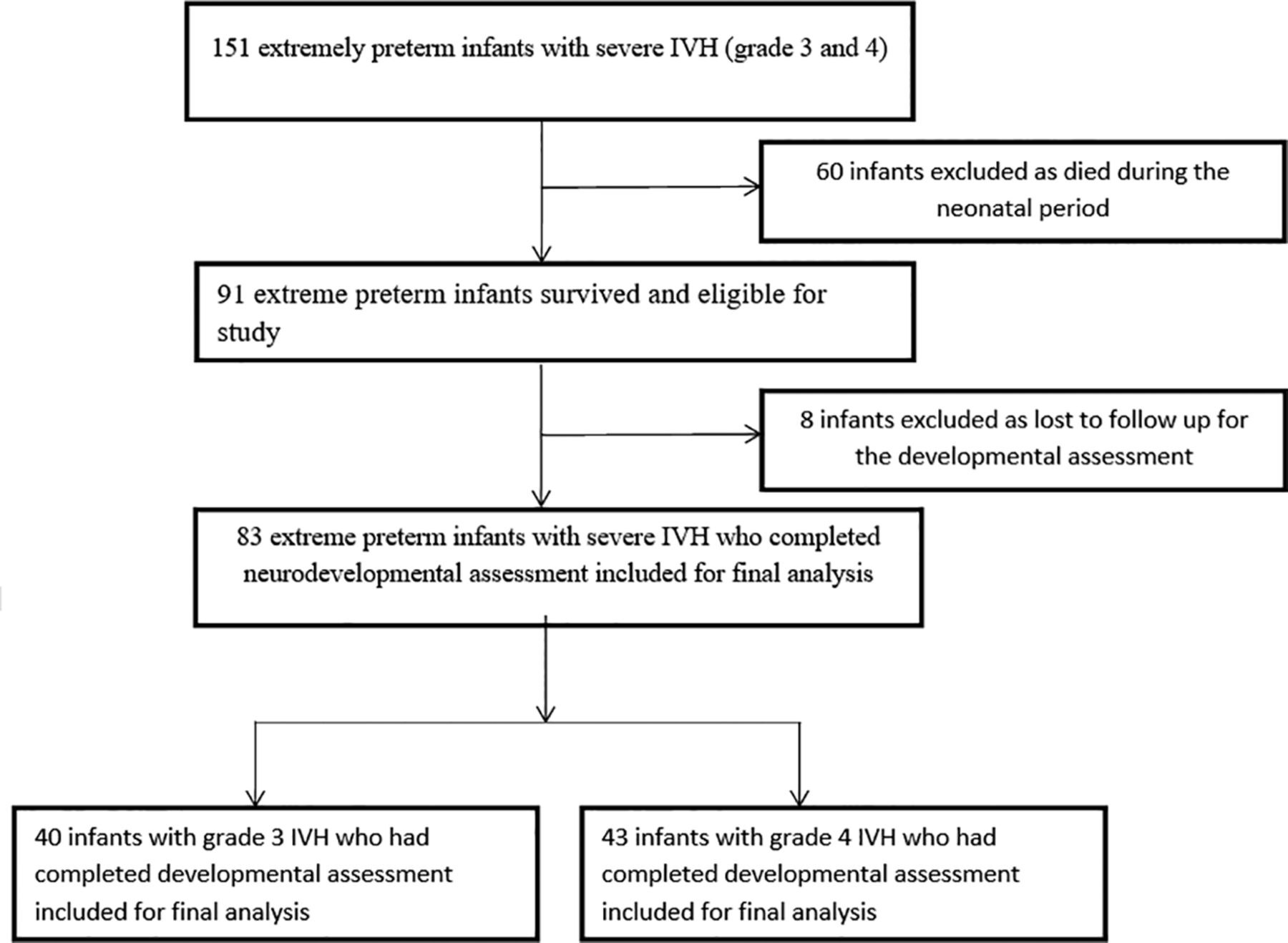
A total of 151 EP infants admitted from January 2006 to December 2016 with a severe (grades 3 and 4) GMH-IVH on the Papile system were included in the study. Of these, 60 infants were excluded from analysis because they died during their NICU admission. Of the 91 surviving infants, 83 underwent their 24-month and/or 36-month developmental assessment using standardized tests (BSID-II or Griffiths). The remaining were lost to follow-up despite adequate attempts to contact and engage the families. The flow diagram of the study population is depicted in Fig 2. The demographic characteristics of the study population are depicted in Table 1.

Study flow diagram.
Demographic characteristics of the study population (n = 83) followed up for neurodevelopmental assessments compared with those who died (n = 60) or were lost to follow-up (n = 8)
Developmental assessments showed that 36 (43.37%) children had scores within 1 SD from the test mean, 19 (22.89%) had scores 1–2 SDs below mean, 13 (15.66%) scored 2–3 SDs below mean, and 15 (18.07%) children scored >3 SD below mean. Thirty-four (40.96%) infants were diagnosed with CP, of whom 8 had moderate-to-severe CP (GMFCS > II). The distribution of infants with Papile grade 3 or 4 GMH-IVH, with their corresponding Al-Abdi score and disability-related outcomes are depicted in Table 2. A total of 22 infants (55%) of 40 with grade 3 GMH-IVH had the outcome of “no impairment.” Of the remaining 18 infants with grade 3 GMH-IVH, a majority of 12 infants (66.67%) had mild impairment. Furthermore, there were 43 infants with grade 4 GMH-IVH. Of these infants with grade 4 GMH-IVH, 14 infants (32.5%) had the outcome of no impairment on long-term neurodevelopmental assessment. Among the remaining 29 infants with grade 4 GMH-IVH, 7 infants (24.13%) had “mild impairment.”
Distribution of infants with IVH 3 or 4 Papile grading, with their corresponding Al-Abdi score and impairment showing subtotals and percentages for each Papile grade
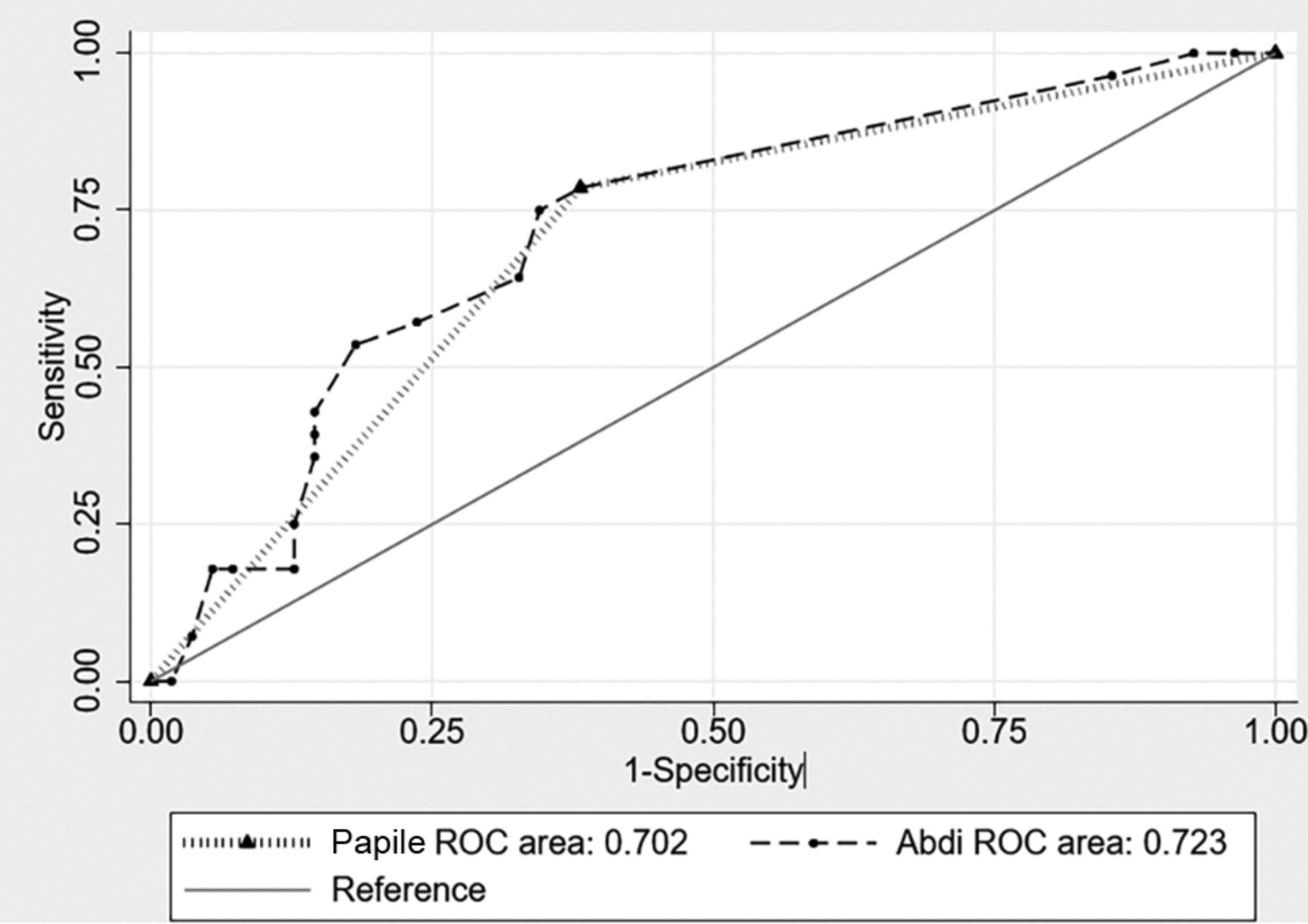
The ROC AUC for the Papile system was 0.702 (95% CI, 0.601–0.802) and 0.723 (95% CI, 0.609–0.835) for the Al-Abdi system (Fig 3). The AUC values between systems were not statistically different in their predictive ability for moderate-to-severe NDI (P = .474). A subsequent comparison of Papile and Al-Abdi models including GA, BW z score, oxygen requirement at 36 weeks, and socioeconomic status (lowest 2 quintiles) also indicated that the 2 systems were comparable in predicting NDI (AUC = 0.749 and 0.751, respectively; P = .943) (Fig 4).

ROC AUC for the Al-Abdi versus the Papile systems.

ROC AUC comparing Papile and Al-Abdi models including GA, BW z score, oxygen at 36 weeks, and socioeconomic status.
Furthermore, the sensitivity, specificity, and correct classification in the prediction of moderate-to-severe NDI of Papile grade 4 were 78.57%, 61.82%, and 67.47%, respectively (Table 3). Corresponding Al-Abdi cutoff scores of 19, 20, 21, and 22 demonstrated increased specificity (range, 76.36%–85.45%) and accurate classification (range, 69.88%–72.29%) to predict moderate-to-severe NDI, albeit with lower sensitivity.
AUC, sensitivity, specificity, and correct classification comparisons of Papile grade 4 and corresponding Al-Abdi scores in the prediction of moderate-to-severe disability
The Al-Abdi scores and Papile grades were significantly lower in the infants that were followed up versus those who were lost to follow-up or died (Al-Abdi: 16 [12–20, 9–35] versus 28 [20–29, 9–35], P < .001; Papile: 43/83 [51.8%] versus 55/68 [80.9%], P < .001).
DISCUSSION
Serial screening cranial ultrasound remains the criterion standard for diagnosing GMH-IVH in preterm infants.20,21 Papile et al8 introduced the very first classification of GMH-IVH in 1978. The older Papile classification system is a descriptive scale involving subjective variation in reporting. It is well-known that all grade 3 and 4 GMH-IVHs are not of the same size, and certainly those resulting in posthemorrhagic ventricular dilation and impact on surrounding brain parenchyma are an important predictor of long-term neurodevelopmental outcomes. Especially, grade 4 GMH-IVH as per the Papile system includes parenchymal extension of the hemorrhage, which is associated with a higher degree of interrater variability in its diagnosis and a higher risk of developing posthemorrhagic ventricular dilation.22 These GMH-IVHs could be small or large, unilateral or bilateral, and can have variable outcomes. This feature reiterates the inaccuracy of labeling them under the same grade as per Papile et al. Recent studies do suggest that the infants with higher grades of GMH-IVH have relatively better long-term prognosis than previously thought.9,23⇓-25
Almost 86% of infants with grade 3 GMH-IVH and 55% with grade 4 GMH-IVH in the present study also had either no or mild impairment. However, the overall attitude of clinicians toward these severe grades of GMH-IVH continues to be pessimistic with “redirection of care” being frequently offered to parents with unsure long-term outcomes.9 This status quo highlights the need for an objective assessment-based classification system to overcome the limitations of the Papile system. There is an urgent need to reclassify the “umbrella” terminologies of grades 3 and 4 GMH-IVH with subtypes among them. An objective scoring system with associated prognostic outcomes for each score under each grade would be very useful while counseling parents about their decision regarding redirection or continuation of care of these EP infants. The Al-Abdi scoring system based on the previously validated Bassan zones for periventricular hemorrhagic infarction provides a feasible alternative. Our results showed that the Al-Abdi and Papile scoring systems were comparable for predicting NDI in EP infants with severe grades of GMH-IVH (Figs 3 and 4 and Table 3).
In a previous study published by Al-Mouqdad et al,14 it was concluded that the newer Al-Abdi classification system was superior to the Papile grading system in predicting NDI at 3 years’ corrected age. Their study included 183 preterm infants with any grade of GMH-IVH. Of these, 79 infants had grade 3 or 4 GMH-IVH. The authors also concluded that an Al-Abdi score of 11 had the best balance between sensitivity (∼90%) and specificity (∼90%) to predict NDI.14 The present study found that an Al-Abdi score of 16 had the best balance between sensitivity (∼80%) and specificity (∼60%). This could probably be explained by the inclusion of lower grades of GMH-IVH in the study by Al-Mouqdad. Additionally, the Al-Abdi system had higher specificity for scores above 20, with an increased accuracy of classification to predict moderate-to-severe NDI in the present study. Thus, it may be useful in prognosticating these infants with objective assessment criteria. It can also aid the health care providers and parents alike with their decisions regarding redirection of care for these infants.
Merhar et al12 assessed the laterality of GMH-IVH in determining neurodevelopmental outcomes at 18–22 months’ corrected age in 166 infants with extremely low birth weights. They used multivariable linear and logistic regression models to determine the impact of laterality and grade of GMH-IVH and other clinical variables to predict scores on standardized developmental assessments. They concluded that bilateral (compared with unilateral) GMH-IVH significantly impacted neurodevelopmental outcome only in infants with grade 4 hemorrhage. Infants with bilateral grades 1–3 GMH-IVH have similar rates of NDI and similar mean Bayley mental and physical development index scores as infants with unilateral grades 1–3 GMH-IVH.12
Similarly, an attempt was made to provide an objective grading system for periventricular hemorrhagic infarction (PVHI) by Bassan et al.10 They classified PVHI into 4 grades (0–3), depending on whether it was bilateral or unilateral, its extent on the worst side, and whether there was a midline shift involved. This retrospective study included 30 preterm infants with median GAs and BWs of 27 weeks (range, 24.9–30.9 weeks) and 937.5 g (range, 653–1335 g), respectively; neurodevelopmental outcomes at a median age of 30 months’ corrected GA were assessed to validate the scoring system. The authors concluded that their PVHI severity scoring system using cranial sonography “could improve the clinician’s ability to counsel parents regarding life support decisions and target early intervention strategies.”10
The strengths and limitations of our study need to be discussed. Complete blinding of the radiologists to clinical and neurodevelopmental data for the included EP infants, comprehensive neurodevelopmental data across a decade with minimal loss to follow-up (5.29%) for infants with severe GMH-IVH, and the use of robust statistical methods to control for confounders with an impact on NDI such as GA, BW z score, oxygen at 36 weeks, and socioeconomic status were strengths of our study. The retrospective design, data from a single tertiary level neonatal unit, and small sample size with inclusion of only EP infants with severe grades (3 and 4) of GMH-IVH are few of the limitations of the present study. The small sample may have limited the ability of our study to contribute to more meaningful interpretation of individual Al-Abdi scores in terms of specificity and sensitivity for the higher grades of GMH-IVH. However, this is a very comprehensive data collection of the long-term outcomes of extremely preterm infants with severe GMH-IVH.
Another limitation was that infants assessed at different ages (24 and 36 months) and with different methods (BSID-II and Griffiths) were analyzed together. The exclusion of those infants who died during the neonatal period could be an additional limitation. This was deemed appropriate because many of these infants were offered redirection of care toward a palliative approach, especially those with bilateral, higher grades of GMH-IVH (grades 3 and 4). Hence, they could not be assessed for their long-term developmental assessments with different combinations of higher grades of GMH-IVH. This issue would not have allowed an appropriate comparison of the 2 grading systems in predicting neurodevelopmental impairment. Finally, the possibility of interreporter variability between the radiologists, specifically when differentiating between grades 2 and 3, cannot be excluded.
CONCLUSIONS
The Al-Abdi classification system is comparable with the existing Papile classification system to predict the neurodevelopmental impairment for extremely preterm infants with grade 3 and 4 GMH-IVH. In fact, the higher Al-Abdi scores are even more specific and accurate at predicting NDI, a feature that could prove useful for the neonatal teams and the parents in their decision regarding the continuation of care or redirection to palliative care. However, multicentric prospective larger studies including all grades of GMH-IVH are recommended to ascertain the validity of the individual Al-Abdi scores in predicting NDI and/or death before they could be approved for regular usage.
Acknowledgments
The authors wish to thank Professor Abhay Lodha (Department of Pediatrics and Community Health Sciences, Cumming School of Medicine, University of Calgary, Canada) and Dr Sameer Al-Abdi (Neonatologist, King Abdulaziz Hospital, Al-Ahsa, Saudi Arabia) for their kind help in providing Fig 1 to better explain the Al-Abdi score.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received September 1, 2021.
- Accepted after revision January 1, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.