
Abstract
BACKGROUND AND PURPOSE: The rate of abnormal intracranial MR imaging findings including subdural collections and dural enhancement after recent lumbar puncture is not known. The purpose of our study was to examine the intracranial MR imaging findings after recent image-guided lumbar puncture.
MATERIALS AND METHODS: Patients who underwent contrast-enhanced MR imaging of the brain within 7 days of a CT-guided lumbar puncture between January 2014 and April 2021 were included. Contrast-enhanced MR images were reviewed for diffuse dural enhancement, morphologic findings of brain sag, dural venous sinus distension, and subdural collections.
RESULTS: Of the 160 patients who met the inclusion criteria, only 6 patients (3.9%) had new diffuse dural enhancement, though none had dural enhancement when the MR imaging was within 2 days of lumbar puncture. All 6 patients with dural enhancement had small, concurrent subdural collections. Two additional patients had subdural collections, for a total of 5.2% of our population.
CONCLUSIONS: Our study is the first to examine intracranial MR imaging after recent lumbar puncture and has 2 key findings: First, 5.2% of patients had small, bilateral subdural collections after recent lumbar puncture, suggesting that asymptomatic subdural collections after recent lumbar puncture are not atypical and do not require further work-up. Additionally, when MR imaging was performed within 2 days of lumbar puncture, none of our patients had diffuse dural enhancement. This argues against the commonly held practice of performing MR imaging before lumbar puncture to avoid findings of dural enhancement, and should not delay diagnostic work-up.
ABBREVIATIONS:
- LP
- lumbar puncture
- SIH
- spontaneous intracranial hypotension
- WBC
- white blood cell
MR imaging findings after lumbar puncture (LP) have not been thoroughly studied. The incidence of diffuse dural enhancement within 30 days after lumbar puncture has been described,1,2 but no prior studies have focused on the incidence of abnormal MR imaging findings immediately after LP. The concern for possible dural enhancement after LP often directs providers to perform MR imaging before LP—a paradigm that can lead to diagnostic and management delays.2
The commonly accepted mechanism causing post-LP dural enhancement is a CSF leak from the puncture site, which leads to low CSF volume and subsequent venous engorgement within the dura per the Monro-Kellie hypothesis.3 Additional intracranial findings associated with spontaneous intracranial hypotension (SIH) in the setting of LP, including subdural collections, are rare and have not been studied except for several case reports.4⇓⇓⇓⇓⇓-10
The purpose of our study was to identify immediate post-LP imaging findings including the frequency of dural enhancement as well as other findings associated with SIH.
MATERIALS AND METHODS
We retrospectively reviewed 2319 patients who underwent an image-guided LP between January 2013 and April 2021. One hundred sixty patients had contrast-enhanced MR imaging of the brain within 7 days of the procedure and were included in our study. All LPs were CT-guided. The indications for the MR imaging and LP were reviewed, as well as infectious, inflammatory, and neoplastic comorbidities that could explain the dural enhancement. Routine CSF evaluation was also reviewed.
All MR imaging studies were reviewed by a neuroradiology fellow (I.T.M.), with equivocal findings additionally reviewed by a neuroradiologist with 4 years’ experience (J.E.V.-M.). This review included any pre-LP MRIs to assess pre-existing findings. In addition to dural enhancement, we evaluated imaging findings associated with CSF hypotension: morphologic findings of brain sag, dominant transverse sinus venous distension,11 and subdural fluid collections.12 A mamillopontine distance of <5.5 mm was used as a quantitative marker of brain sag.13 Basic statistical analysis (mean [SD]) was performed with Excel (Microsoft).
RESULTS
All Patients
The mean age of the 160 patients included in this study was 54.8 (SD, 17.6) years (range, 21–93 years). Sixty-nine patients (43.1%) were women. The mean time from LP to MR imaging was 2.1 days. We used the following needle sizes: 22-ga Quincke tip (BD Medical) (144 patients), 20-ga Quincke tip (10 patients), 17-ga Tuohy (B. Braun Medical Inc.) (5 patients), and 25-ga Quincke tip (1 patient). One hundred fifty-six patients had CSF removed, with a mean volume of 15.6 (SD, 6.8) mL. Opening pressure was recorded in 54 patients, with a mean of 20.3 (SD, 8.9) cm H2O (range, 7–43 cm H2O). Seven patients had pre-existing dural enhancement before LP. Of the remaining 153 patients, 6 patients (3.9%) had diffuse dural enhancement (Table 1).
Contrast-enhanced MR imaging findings of patients who underwent imaging within 7 days of an image-guided LPa
Patients with Subdural Collections
Seven patients had subdural collections before LP. Of the remaining 153 patients, 8 patients (5.2%) had small bilateral subdural collections with a mean of 3.1 days between LP and MR imaging (range, 0–6 days) (Table 2). The mean age was 58.8 years (range, 35–71 years). All procedures used a 22-ga Quincke tip needle for the LP with a mean of 12.3 mL of CSF removed (range, 6–16 mL). The opening pressure was obtained in 2 patients (13 and 14 cm H2O). Of the 8 patients, 6 had diffuse dural enhancement (Figs 1 and 2). Of the 7 excluded for prior subdural collections, 2 collections were at the site of prior craniotomies, 1 patient had diffuse dural metastases, 2 had thrombocythemia, 1 had coccidioidal meningitis, and 1 collection was idiopathic. None of these patients had a known connective tissue disorder.
Eight patients who had subdural collections on MR imaging within 7 days after LPa

A 42-year-old woman (patient 2) with B-cell acute lymphoblastic leukemia who had an LP for intrathecal chemotherapy followed by MR imaging 4 days later. CSF did not show signs of infection, inflammation, or malignancy. A, T1-weighted postcontrast coronal MR imaging shows smooth, diffuse dural enhancement. B, FLAIR coronal MR imaging shows small bilateral subdural fluid collections without mass effect.

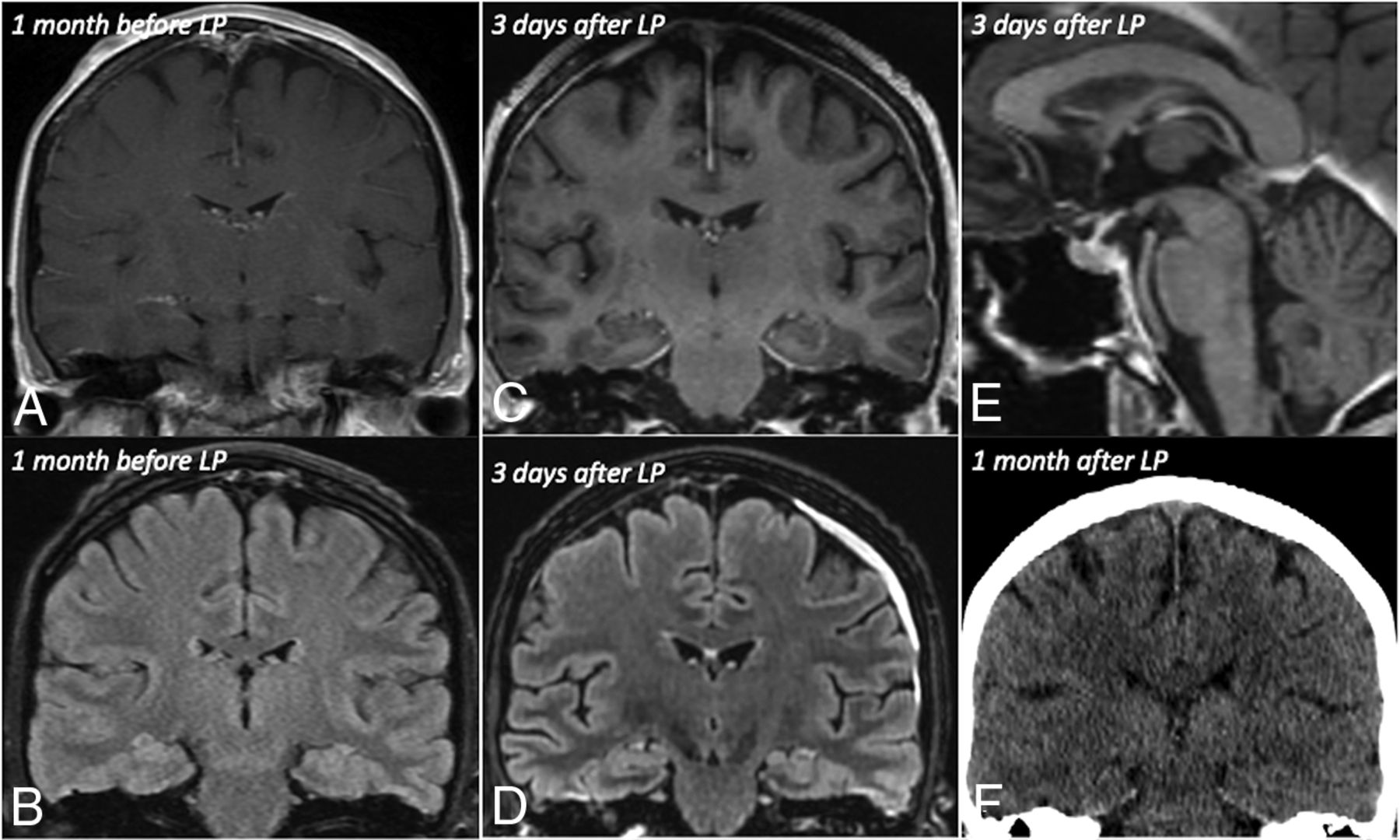
A 69-year-old man (patient 5) with a history of multiple myeloma underwent an LP followed by MR imaging 3 days later. Coronal T1-weighted postcontrast (A) and FLAIR (B) images 1 month before LP do not show subdural collections or dural enhancement. However, 3 days after the LP, MR images show smooth diffuse dural enhancement on coronal T1-weighted postcontrast imaging (C) and a left frontal convexity subdural fluid collection on coronal FLAIR imaging (D) but no morphologic findings of brain sag on T1-weighted sagittal imaging (E). F, Coronal reformatted CT 1 month after LP shows resolution of the subdural fluid collection.
Patient 1.
A 35-year-old man who was hospitalized for a neutropenic fever in the setting of mycosis fungoides that involved the superficial soft tissues of the face with diffuse lymphadenopathy. MR imaging performed 4 days after LP demonstrated brain sag, venous distension, small subdural fluid collections, and diffuse dural enhancement, which were not present on an MR imaging 24 days before LP. However, since the comparison MR imaging, the patient had 4 additional LPs. The patient reported a long-standing headache on admission that predated the comparison MR imaging with normal findings. One week after the last LP, the patient was evaluated for a blood patch on the basis of the persistent headache and abnormal MR imaging findings; however, this was not performed secondary to a large skin ulcer over the lumbar spine. The headache improved without a blood patch by day 11 after LP. CSF analysis showed elevated glucose (93 mg/dL) and total protein levels (185 mg/dL) with a normal white blood cell (WBC) count and benign CSF findings on cytopathology analysis.
Patient 2.
A 42-year-old woman presented for treatment of B-cell acute lymphoblastic leukemia (Fig 1). She had an LP 15 days before the LP included in our study. MR imaging performed 4 days after the LP demonstrated venous distension, small subdural fluid collections, and diffuse dural enhancement without brain sag. She did not have comparison MR imaging. The patient reported a headache the day after the LP; however; this resolved by day 5 without a blood patch. CSF had a normal total protein level, WBC count, and cytology findings.
Patient 3.
A 54-year-old man with a history of a renal transplant who presented with fever of unknown origin. He did not have a prior LP. MR imaging performed 3 days after LP demonstrated diffuse dural enhancement and small subdural fluid collections without venous distension or brain sag. Comparison MR imaging was not available. He remained in the hospital for 21 days after his LP and did not report a headache or require a blood patch. CSF had a normal total protein level and WBC count.
Patient 4.
A 61-year-old woman admitted for a prolonged spinal infection who underwent an LP and MR imaging for new-onset encephalopathy. Given the extensive spinal infection, the CT-guided LP was performed via a C1–C2 puncture. There was no history of a prior cervical or lumbar puncture. MR imaging performed on the same day as the C1-C2 puncture demonstrated small subdural fluid collections in addition to separate extra-axial blood at the puncture site without brain sag, venous distension, or diffuse dural enhancement. MR imaging 35 days before the C1-C2 puncture did not show subdural fluid collections. The patient did not have a headache or require a blood patch throughout the remainder of the hospitalization, which lasted 23 days after the C1-C2 puncture. CSF had normal total protein level and WBC count.
Patient 5.
A 69-year-old man was admitted for treatment of multiple myeloma (Fig 2). There was no history of LP. MR imaging performed 3 days after the LP demonstrated diffuse dural enhancement and small subdural fluid collections without brain sag or venous distension. These findings were new on the basis of comparison MR imaging 40 days prior. CSF had normal total protein levels, WBC count, and cytology findings. He did not have a headache or require a blood patch during the remaining 38 days of his hospitalization.
Patient 6.
A 69-year-old woman underwent an LP for intrathecal chemotherapy in the setting of mixed phenotype acute leukemia. Within the 30 days before her LP, she had 5 additional LPs. The MR imaging performed 1 day after the LP demonstrated small subdural fluid collections without brain sag, venous distension, or diffuse dural enhancement. These findings were new compared with the most recent comparison MR imaging 44 days prior. CSF had a normal total protein level, WBC count, and cytology findings. She did not have a headache or require a blood patch during the remaining 48 days of her hospitalization.
Patient 7.
A 69-year-old man presented with new left abducens nerve palsy with an acute right MCA territory infarct and was found to have newly diagnosed metastatic lung cancer. A bedside LP was attempted before the image-guided LP. MR imaging performed 6 days after the LP demonstrated diffuse dural enhancement and small subdural fluid collections without brain sag or venous distension. These findings were new compared with the most recent comparison MR imaging 16 days prior. CSF demonstrated elevated total protein level (118 mg/dL) without an elevated WBC count. CSF cytology was not performed. He did not have a headache during the 17 days before being transitioned to comfort care in the setting of metastatic carcinoma.
Patient 8.
A 71-year-old man presented with altered mental status in the setting of atypical chronic myeloid leukemia. A bedside LP was attempted before the image-guided LP. The MR imaging performed 4 days after the LP demonstrated diffuse dural enhancement and small subdural fluid collections without brain sag or venous distension. These findings were new compared with the most recent comparison noncontrast MR imaging 24 days prior, though comparison for dural enhancement was limited because there was no overt dural thickening. CSF had a normal total protein level and WBC count. He did not have a headache or require a blood patch during the remaining 13 days of his hospitalization.
MR Imaging Immediately after LP
Of the patients who had MR imaging performed on the same day (40 patients), 1 day after (35 patients), and 2 days after LP (10 patients), none had new diffuse dural enhancement or morphologic findings of brain sag. Two patients had venous distension not seen on prior imaging. Seven patients had subdural collections; however, 5 were unchanged from pre-LP MR imaging.
High-Volume Lumbar Puncture
Six patients (3.9%) had at least 30 mL of CSF removed. Of these patients, the mean CSF removed was 33 mL (range, 30–40 mL). None of these patients had dural enhancement, subdural collection, venous distension, or brain sag.
Intrathecal Chemotherapy
Thirteen patients underwent LP for the administration of intrathecal chemotherapy, one of whom had diffuse dural enhancement (Table 2).
DISCUSSION
Our study found that of patients undergoing brain MR imaging within 7 days of LP, 5.2% of patients had small subdural collections. Subdural collections after LP have been previously reported in case reports in symptomatic patients,4⇓⇓⇓-8 without prior studies to describe the incidence. Additionally, while 3.9% of our total population had dural enhancement, none of the patients who underwent MR imaging within 2 days of LP or who had large-volume CSF removal had dural enhancement.
These 2 findings are important but for different reasons. Previous studies have examined the incidence of dural enhancement after LP; however, they focused on MR imaging examinations that occurred within 1 month after LP. Mittl et al1 found that 11 patients of 97 had diffuse dural enhancement within 1 month after LP; however, 10 of the 11 patients had a comorbidity to explain the findings. Wesley et al2 studied 77 patients who underwent an MR imaging within 30 days after LP and found only a single case of unexplained dural enhancement in a patient who underwent a large-volume tap. Our study is the first to focus on patients who underwent MR imaging within 2 days of LP, none of whom had dural enhancement. This finding suggests that the commonly held practice of performing an MR imaging before LP to avoid findings of dural enhancement should not delay the diagnostic work-up.
Furthermore, we are the first study to examine the rate of subdural collections after LP. Prior authors have demonstrated subdural collections in 20%–45% of patients with SIH.14 In the setting of SIH, the tearing of the bridging veins or rupture of the dilated thin-walled blood vessels in the subdural zone has been proposed as the causative mechanism.15 While this is the most likely mechanism in our patients, 2 of our patients had isolated subdural collections without additional SIH findings. Tosaka et al12 examined serial images of 8 patients with SIH and found that dural enhancement resolved before the subdural collections and could be a possible explanation in our study. De Noronha et al16 described a case series of patients with SIH, of whom 2 patients had subdural collections without dural enhancement. The mechanism that leads to subdural collections without dural enhancement is not well-understood, but it could be related to pre-existing susceptibility of the cortical vessels that places them at greater risk of damage in the setting of SIH. Additionally, the timing of dural enhancement in SIH has been shown to be variable, and some patients can take a longer time to develop dural enhancement than the duration our study.17 Most interesting, of the 8 patients with subdural collections, 3 had a prior image-guided LP within the past month (ranging from 1 to 5 prior LPs) and 2 had failed bedside LP attempts. This scenario further supports CSF leakage and SIH as the etiology for the abnormal MR imaging findings.
Our study has several limitations, starting with its retrospective nature. Second, our patients underwent an LP with image guidance; however, this in line with recent Medicare trends.18 Additionally, none of our patients received an epidural blood patch, compared with a previously reported 4.2% rate with image-guided LP.19 Given this discordance, it raises the question of whether our technique and sample size are reflective of the greater population. All our patients underwent CT guidance for their LP, reflecting our group practice. In theory, the improved needle localization of CT over fluoroscopy would allow a less traumatic procedure with possibly fewer dural punctures. In this case, our study could underrepresent the incidence of abnormal MR imaging findings. However, the benefits of CT guidance help with navigation around degenerative osteophytes rather than changing the number of dural punctures. Final limitations that may affect the generalizability of our study include the selection of the needle size (most of our cases involved a 22-ga spinal needle) and age (pediatric patients were excluded).
CONCLUSIONS
Our study is the first to examine the intracranial MR imaging findings after recent CT-guided LP and has 2 key findings: First, 5.2% of patients had small, bilateral subdural collections after recent LP, suggesting that subdural collections are not atypical and, if asymptomatic, do not require further work-up. Additionally, when MR imaging was performed within 2 days of LP, none of our patients had diffuse dural enhancement. This finding argues against the commonly held practice of performing MR imaging before LP to avoid findings of dural enhancement, and it should not delay diagnostic work-up.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received January 16, 2022.
- Accepted after revision March 4, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}