
Abstract
BACKGROUND AND PURPOSE: Stent-assisted coiling may improve angiographic results of endovascular treatment of unruptured intracranial aneurysms compared with coiling alone, but this has never been shown in a randomized trial.
MATERIALS AND METHODS: The Stenting in the Treatment of Aneurysm Trial was an investigator-led, parallel, randomized (1:1) trial conducted in 4 university hospitals. Patients with intracranial aneurysms at risk of recurrence, defined as large aneurysms (≥10 mm), postcoiling recurrent aneurysms, or small aneurysms with a wide neck (≥4 mm), were randomly allocated to stent-assisted coiling or coiling alone. The composite primary efficacy outcome was “treatment failure,” defined as initial failure to treat the aneurysm; aneurysm rupture or retreatment during follow-up; death or dependency (mRS > 2); or an angiographic residual aneurysm adjudicated by an independent core laboratory at 12 months. The primary hypothesis (revised for slow accrual) was that stent-assisted coiling would decrease treatment failures from 33% to 15%, requiring 200 patients. Primary analyses were intent to treat.
RESULTS: Of 205 patients recruited between 2011 and 2021, ninety-four were allocated to stent-assisted coiling and 111 to coiling alone. The primary outcome, ascertainable in 203 patients, was reached in 28/93 patients allocated to stent-assisted coiling (30.1%; 95% CI, 21.2%–40.6%) compared with 30/110 (27.3%; 95% CI, 19.4%–36.7%) allocated to coiling alone (relative risk = 1.10; 95% CI, 0.7–1.7; P = .66). Poor clinical outcomes (mRS >2) occurred in 8/94 patients allocated to stent-assisted coiling (8.5%; 95% CI, 4.0%–16.6%) compared with 6/111 (5.4%; 95% CI, 2.2%–11.9%) allocated to coiling alone (relative risk = 1.6; 95% CI, 0.6%–4.4%; P = .38).
CONCLUSIONS: The STAT trial did not show stent-assisted coiling to be superior to coiling alone for wide-neck, large, or recurrent unruptured aneurysms.
ABBREVIATIONS:
- CA
- coiling alone
- DSMC
- Data and Safety Monitoring Committee
- RR
- relative risk
- SAC
- stent-assisted coiling
- UIA
- unruptured intracranial aneurysm
The use of stents for the treatment of unruptured intracranial aneurysms (UIAs) was first approved in the United States in 2002 as a Humanitarian Device Exemption. The initial indication was to mechanically assist the coiling of wide-neck (≥4 mm) aneurysms not amenable to endovascular or surgical treatment.1,2 Subsequently, clinical usage has expanded to all types of aneurysms.3⇓⇓⇓⇓⇓⇓⇓⇓-12 While coiling is strictly an intrasaccular treatment, stents are deployed in the artery bearing the aneurysm. Antiplatelet regimens are therefore necessary to prevent arterial thromboembolic complications, rendering the use of stents problematic in recently ruptured aneurysms.13 There may be benefits to the use of stent-assisted coiling (SAC), in addition to mechanically preventing coil protrusion into the parent artery during the coiling procedure, which may improve the long-term angiographic results of endovascular treatments such as a flow-diverting effect14⇓-16 or better healing due to the provision of a scaffold for neointimal closure of the neck.17 However, these potential benefits were not observed in experimental models.18 Whether SAC increases procedural risks or improves long-term angiographic results has not been convincingly shown despite multiple case series and meta-analyses published during 20 years.3⇓⇓⇓⇓⇓⇓⇓⇓-12 A randomized trial comparing the results of coiling with or without stent placement has never been published.
The Stenting in the Treatment of Aneurysm Trial (STAT) was launched in 2011 to provide a clinical research context for the use of SAC in UIAs.19 The trial compared a policy of coiling alone (CA) versus the use of a self-expandable stent (any stent, not a flow diverter) in addition to the coiling procedure. The primary hypothesis of the trial was that in patients with aneurysms prone to recurrence, SAC would decrease the proportion of patients reaching “treatment failure,” a composite clinical and angiographic primary outcome measure that included aneurysmal rupture or retreatment during follow-up or a recurrent or residual aneurysm on follow-up angiography at 12 months. We here report the final results of the trial.
MATERIALS AND METHODS
This report follows the Consolidated Standards of Reporting Trials (CONSORT) recommendations.20 STAT was an investigator-led, multicenter randomized controlled trial integrated into clinical practice. The trial proposed randomized allocation to SAC or CA in patients eligible for both options. There were 4 participating centers (Montreal, Ottawa, and Edmonton in Canada, and Brest in France). All sites received institutional review board approval. The protocol was published,19 and the trial was registered at http://www.clinicaltrials.gov number NCT01340612.
Patients
All patients were 18 years of age or older with a life expectancy of at least 2 years. Patients had at least 1 UIA prone to recurrence, defined and categorized at the time of registration before randomization as a large (≥10 mm) aneurysm (STAT-1), a recurrent aneurysm after previous coiling (STAT-2), or a wide-neck (≥4 mm) aneurysm of <10 mm (STAT-3). There were few exclusion criteria: 1) absolute contraindications to endovascular treatment, anesthesia, or the use of dual antiplatelet regimens; 2) the presence of other aneurysms requiring treatment during the same session; 3) the presence of an associated cerebral arteriovenous malformation; 4) recently ruptured aneurysms (<3 months); and 5) the presence of a recurring, previously stented aneurysm. Screening logs of all potentially eligible patients with UIAs were not required per protocol. All patients signed an informed consent form.
Randomization and Masking
SAC or CA was randomly allocated (1:1) using a Web-based platform assuring concealment of the allocation. The randomized allocation was stratified according to the STAT1–3 subgroups and minimized for the type of coils to be used (platinum or second generation). Patients, interventionists, and outcome assessors were not blinded to treatment assignment.
Interventions and Follow-up Tests and Visits
Coiling with or without stent placement was performed according to standards of practice, with the patient under general anesthesia. Antiplatelet and anticoagulation regimens and testing for platelet inhibition were prescribed according to routine practice at each site. Details regarding the endovascular technique; type of coils; use of adjunctive techniques such as balloon remodeling (routine in STAT centers for large or wide-neck aneurysms); whether the stent was deployed before or following coiling; the use of multiple stents; and posttreatment medical management decisions were left to the discretion of the treating physicians. A stent could be used as a bailout maneuver in patients allocated to CA if this was judged appropriate by the treating physician, to ensure the safety of patients. Similarly, the physician could choose not to use the stent in patients allocated to SAC when it was judged impossible or dangerous at the time of the procedure.
Follow-up tests and visits were limited to those considered clinically indicated, such as neurologic examinations, brain imaging studies, and a functional assessment according to the mRS score at discharge, 1 month, and 12 (±3) months. Follow-up angiography (invasive or noninvasive) at 12 (±3) months was considered standard of practice.
Data capture and management through secure servers (MedSciNet; https://medscinet.com/about.aspx) were in compliance with good clinical practice requirements. Case report forms were simple, and the data collected were parsimonious, to facilitate completion by care personnel, because no financial compensation was provided to participating centers.
Primary and Secondary Outcome Measures
The primary end point of the 2011 protocol was the incidence of angiographic recurrences at 12 (±3) months, defined as the following: 1) an angiographic recurrence of the lesion, as judged by an independent core lab (composed of 2 raters) according to a previously published classification;21 2) an episode of intracranial bleeding; or 3) retreatment of the same lesion by endovascular or surgical means during the follow-up period.19 Furthermore, the protocol stipulated that “recurrences would be recorded (present or absent) as they are discovered, at the follow-up assessment (12 ± 3 months), as clinical symptoms appear at any time, or at time of death.”19
Because this definition lacked precision and may not be ascertainable in some patients, the primary outcome was modified in July 2021, after consulting with the Data and Safety Monitoring Committee (DSMC) but before any data examination, to be in line with other endovascular trials.22⇓-24 Two other components have been added to the composite primary outcome, treatment failure (initial treatment failure using any device and treatment- or aneurysm-related death or dependency precluding follow-up angiography). If the coiling procedure was not feasible, for example due to coil instability, the physician had the option of using a stent, a use that was not considered a failure of the initial treatment (but was counted as a crossover in “as-treated analyses”). One primary poor outcome was attributed per patient. When a patient met >1 of the criteria, the following hierarchical order was prespecified to classify the patient for final analyses: death or mRS 3–5 (from any cause within 30 days of the intervention and from related causes during follow-up) > aneurysm rupture during follow-up > retreatment during follow-up > initial treatment failure (defined as the inability to perform endovascular treatment) > major recurrence or residual aneurysm at imaging follow-up (3–12 months) as adjudicated by an independent core laboratory of 2 neuroradiologists blinded to treatment groups and according to a previously validated classification.25,26
Secondary outcomes included the individual components of the composite primary outcome: the mRS score at discharge and 12 months posttreatment; the success in occluding the aneurysm at the end of the procedure; perioperative complications (ischemic strokes and intracranial hemorrhages within 31 days of the intervention and during follow-up); angiographic results at 12 months; length of hospital stay (number of days); discharge disposition (home, other hospital, rehabilitation facility; death); and retreatment of the index aneurysm at any time.
Hypotheses and Number of Patients
The 2011 protocol planned for the recruitment of 600 patients.19 This number was based on 2 hypotheses: The primary efficacy hypothesis was that SAC would decrease angiographic recurrences by 20% at 12 months and a total sample size of 536 patients would allow the detection of such a difference with a power of 80% and an error of 0.0125 (to account for subgroup analyses for the 3 main categories of lesions: large, wide neck, and recurrent aneurysms). The secondary safety hypothesis was that the use of intracranial stent placement would not double the number of dead or dependent patients (mRS > 2) from 6% to 12% at 12 months. In July 2021, before any knowledge of the data, the steering committee (SC), in agreement with the DSMC, dropped the safety hypothesis and modified the primary efficacy hypothesis: SAC was hypothesized to decrease treatment failures from 33% to 15%, which would require approximately 200 patients (88 patients per group; power of 80% and α of 5%, plus 10% to account for crossovers and losses to follow-up). Details are provided in the Online Supplemental Data.
Trial Interruption
On August 31, 2021, after a blinded examination of interim results, the DSMC recommended trial continuation. However, in September 2021, ten years after the recruitment of the first patient, the SC decided to finalize and report the trial.
Statistical Analyses
Blinded data were examined at prespecified intervals by an independent DSMC, composed of an interventional neurologist, a dual-trained neurosurgeon, and a statistician; but no hypothesis testing was performed.
Descriptive statistics on demographic variables and preoperative data are provided to compare the 2 groups at baseline. Means, SDs, medians, and ranges are presented for quantitative variables, and frequency tables for categoric variables. Primary safety and efficacy outcomes are described using percentages and 95% CIs. The intent-to-treat analyses for the primary efficacy hypothesis were performed on available observations. The relative risks (RRs and 95% CIs) were estimated using a generalized estimating equation with a binomial distribution and a log-link function. The groups were not different with respect to risk factors for poor outcomes, and no adjustments for residual confounding factors were made.
The analyses of interaction between prespecified subgroups of interest and treatment were made by adding subgroup variables and interaction in generalized estimating equation models. Patient and aneurysm subgroups were examined as prespecified in 2011, regardless of the results of tests for interaction. Subgroup results according to STAT 1–3 categories indicated at the time of registration, according to aneurysm size (<10 mm or ≥10 mm), neck size (<4 mm or ≥4 mm), and location (posterior circulation and anterior circulation subdivided into carotid, anterior cerebral artery, and MCA aneurysms) are reported. As-treated exploratory analyses (defined as coiling with or without any attempt or use of stent placement, regardless of treatment allocation) are also provided. We also explored what results would have been if complete occlusion (rather than the combination of complete and near-complete occlusion) had been used as the criterion for a good angiographic outcome. One adverse event is reported per patient. When a patient had >1 event, we used the most severe to categorize the patient. Analyses were performed using SAS software, Version 9.4 (SAS Institute) and SPSS, Version 26 (IBM) with a significance level of 5%.
Roles of the Sponsor and Funding Source
The trial was sponsored by the Center Hospitalier de l’Université de Montréal. The sponsor had no part in the study design, data collection, analysis, or reporting and no access to the data or source documents. The corresponding author had full access to all the data and had final responsibility for the decision to submit for publication. There was no funding source for this study.
RESULTS
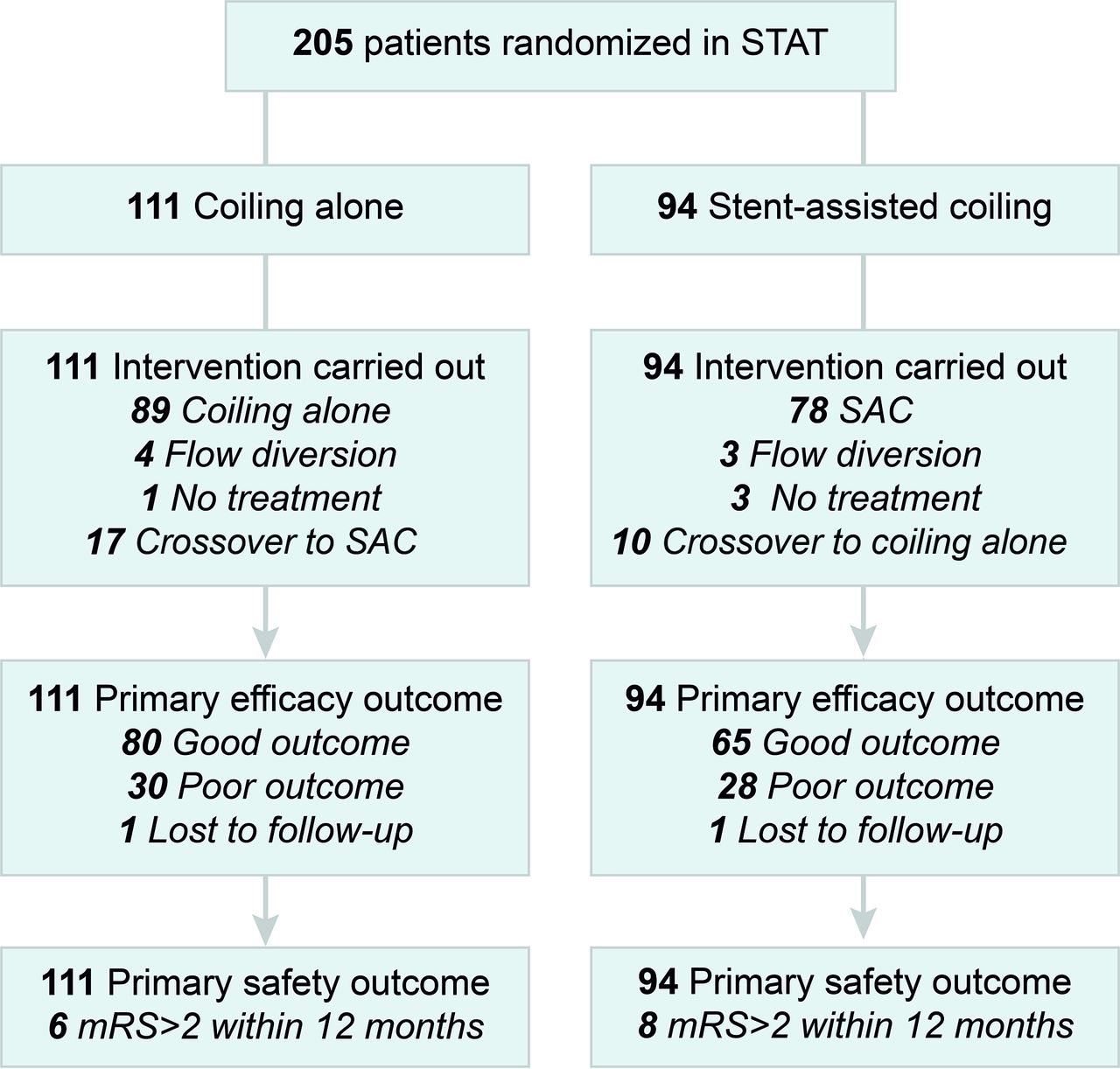
Between August 2011 and August 2021, we recruited 205 patients: Ninety-four were assigned to SAC, and 111 to CA. For each group, the number of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome is illustrated in the trial profile (Fig 1).

STAT participant flow CONSORT diagram.20
The baseline patient and aneurysm characteristics are shown in Table 1. Groups were comparable: Ninety-two (44.9%) patients had small wide-neck aneurysms (STAT-3); 75 (36.6%), a recurrent aneurysm (STAT-2); and 38 (18.5%), a large aneurysm (STAT-1). The most frequent locations were the anterior communicating artery (65; 31.7%), basilar bifurcation (47; 22.9%), and MCA bifurcation (32; 15.6%).
Patient and index aneurysm characteristics
Seventeen of 111 patients (15.3%) allocated to CA underwent SAC, while 10/94 (10.6%) patients allocated to SAC were treated with CA. Technical details regarding treatment for both groups are provided in the Online Supplemental Data. In 4 patients from STAT-2, residual aneurysms were judged too small for any treatment (3 in the SAC arm and 1 in the CA arm). Seven patients were treated with flow diverters (3 in the SAC arm and 4 in the CA arm). Patients allocated to SAC were initially treated with a single (n = 64) or 2 (n = 14) stents. Stents were delivered before coiling in 20/78 (25.6%) and after coiling in 58/78 (74.4%) patients.
The primary outcome is available for 203/205 patients (99%), with 1 patient missing in each group (Fig 1 and Tables 2 and 3). Treatment failure occurred in 28/93 patients allocated to SAC (30.1%; 95% CI, 21.2%–40.6%) compared with 30/110 (27.3%; 95% CI, 19.4%–36.7%) allocated to CA (RR = 1.10; 95% CI, 0.7–1.7; P = .66). Details of each component of the primary outcome in the intent to treat analysis are provided in Table 2.
Primary outcome in intent-to-treat analysis
Secondary outcomes in intent-to-treat analysis
There were no incidences of aneurysm rupture during follow-up. Three patients were retreated (all in the SAC group). Angiographic results at 12 months accounted for most of the primary outcome adjudications (185/203; 91%). Follow-up vascular imaging studies, available in 198 patients (96.6%), were performed by MRA in 135 (68.2%), by catheter angiography in 59 (29.8%), and by CTA in 4 (2%) patients. More patients were followed by catheter angiography in the SAC group (37.2%) than in the CA group (21.6%) (Table 3). The mean time of angiographic follow-up was 14.8 (SD, 9.5) months for patients allocated to SAC, and 13.5 (SD, 5.2) months for patients allocated to CA. The mean time of the follow-up mRS evaluation was 15.3 (SD, 8.0) months for SAC and 15.7 (SD, 10.5) months for CA.
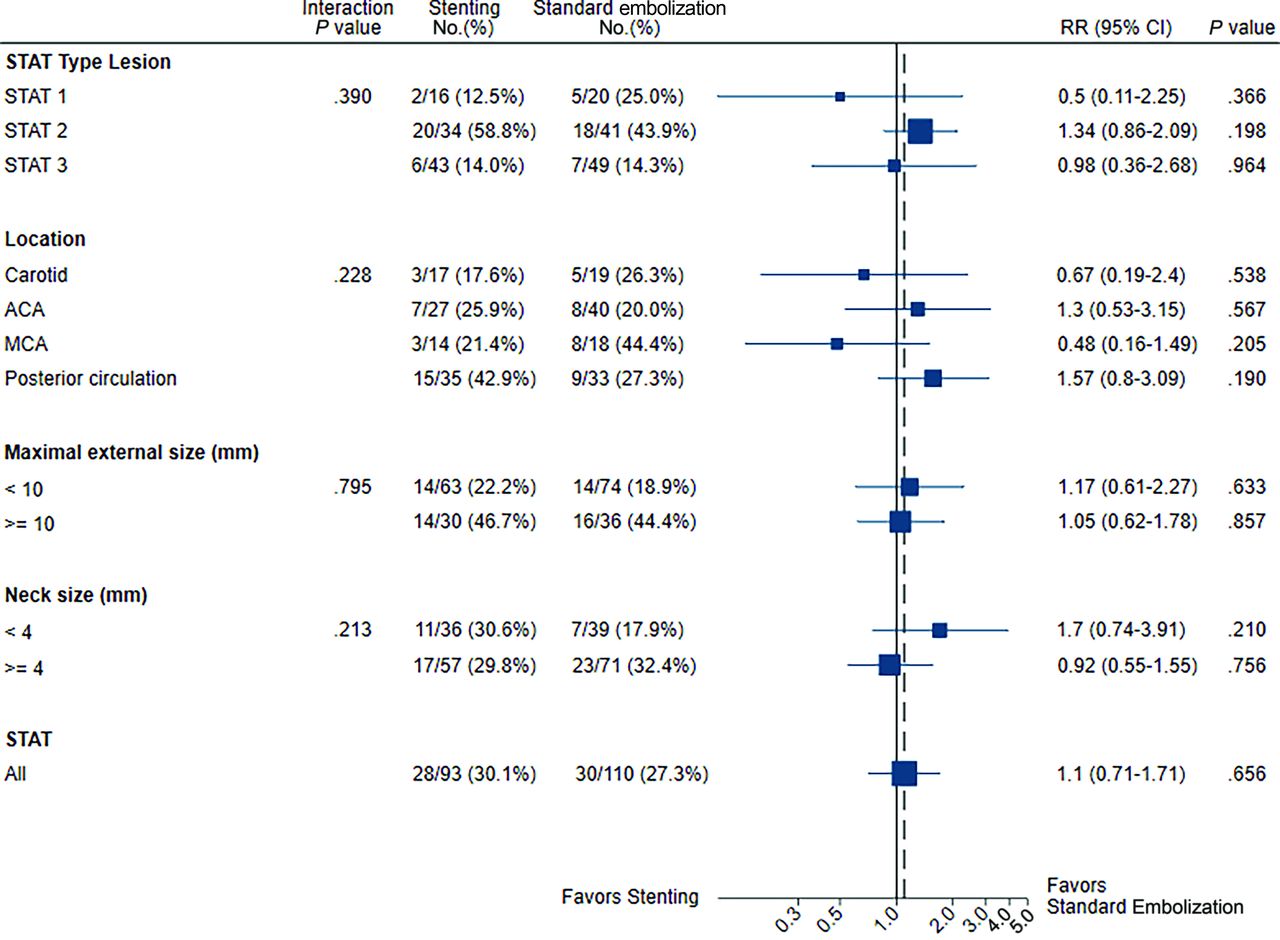
Results for predefined subgroups of interest are illustrated in the forest plot (Fig 2), even though none of the interaction tests were significant.

Subgroup analysis of the primary outcome at 1 year. ACA indicates anterior cerebral artery.
Poor clinical outcomes (mRS > 2) in the intent to treat analysis are detailed in Table 4. A poor clinical outcome (mRS > 2) occurred in 8/94 patients allocated to SAC (8.5%; 95% CI, 4.0%–16.6%) compared with 6/111 (5.4%; 95% CI, 2.2%–11.9%) with CA (RR = 1.6; 95% CI, 0.6–4.4; P = .38). Five deaths were related to treatment complications (2 in the CA and 3 in the SAC arms). Deaths unrelated to the aneurysm or treatment (and not included in the primary outcome measure) were reported in 3 patients (1 in the CA and 2 in the SAC groups). Details of poor clinical outcomes at any time point are provided in the Online Supplemental Data.
Clinical outcomes (mRS > 2 at 12 months) in intent-to-treat analysis
Adverse events occurred in 25/94 (26.6%) patients with SAC and 23/111 (20.7%) with CA (RR = 1.28; 95% CI, 0.78–2.11; P = .323). Cerebrovascular ischemic and hemorrhagic events occurred in 21/94 (22.3%) patients with SAC, and in 18/111 (16.2%) with CA (RR = 1.38; 95% CI, 0.78–2.43; P = .268). Complication rates according to subgroups of interest are provided in the Online Supplemental Data. The test of interaction was significant for aneurysm size (P = .02): complications were more frequent in patient with aneurysms <10 mm allocated to SAC than in those allocated to CA (RR 2.0 ± 0.69 95% CI 1.0–3.9; P = .04).
Results for the secondary outcomes in the intent-to-treat analyses are detailed in Table 3. Secondary outcomes (immediate and 12 month angiographic outcomes, days of hospitalization, discharge disposition, mRS at discharge and at 12 months) were similar between groups. Angiographic results at 12 months were similar (RR 1.1; 95% CI 0.66–1.71; P = .789). Changing the definition of a good angiographic outcome as a complete occlusion did not change results (Online supplemental data).
As-treated analyses included 198/205 patients (97%; seven patients treated with flow diverters were excluded). The primary outcome (treatment failure) occurred in 27/102 patients treated with SAC (26.5%; 95% CI, 18.4%–36.3%) compared with 29/94 (30.8%; 95% CI, 21.9%–41.3%) treated with CA (RR = 0.86; 95% CI, 0.55–1.34; P = .498). Details of each component of the primary outcome are provided in Table 5.
Primary outcome in as-treated analysis
Predefined as-treated subgroup analyses of the primary outcome are detailed and illustrated in the forest plot (Online Supplemental Data). There were no significant interactions, and subgroup results were similar.
In as-treated analyses, all-cause death or dependency at 1 year occurred in 10 of 104 (9.6%) SAC patients and in 4 of 94 CA patients (4.3%) (RR = 2.26; 95% CI, 0.73–9.96; P = .156) (Table 6). Other secondary outcomes (Online Supplemental Data) (immediate angiographic outcomes, days of hospitalization, discharge disposition, and mRS at discharge and at 12 months) were similar between groups.
Clinical outcomes (mRS > 2 at 12 months) in as-treated analysis
As-treated angiographic results at 12 months, categorized as the presence of a residual aneurysm or not, were not significantly different (RR = 0.77; 95% CI, 0.48–1.2; P = .300). SAC was significantly better than CA in as-treated analyses when “complete occlusion” was used as the definition of a good angiographic outcome (RR = 0.74; 95% CI, 0.59–0.94; P = .012) (Online Supplemental Data).
Adverse events (any severity) occurred in 34/104 (32.7%) patients who underwent SAC, compared with 12/94 (12.8%) patients with CA (RR = 2.56; 95% CI, 1.41–4.65; P = .002). Details are provided in the Online Supplemental Data. Ischemic and hemorrhagic events were more frequent in patients who underwent SAC (30/104 [28.8%]) compared with 7/94 (7.4%) patients who received CA (RR = 3.87; 95% CI, 1.79–8.40; P = .001).
DISCUSSION
The Problem of Residual Aneurysms after Coiling
Residual or recurrent aneurysms after coiling occur in 10%–33% of patients.27,28 In ruptured aneurysms, they have been associated with a persistent risk of subarachnoid hemorrhage.27,28 In UIAs, they are more likely to occur in large, wide-neck, and recurrent aneurysms.23 In the context of a preventive treatment against ruptures, recurrences lead to a number of clinical consequences, such as routine angiographic surveillance of nearly all patients and retreatment in 5%–15%29 (even up to 25% of patients at 10 years in some series).30 Potentially more effective coils have been developed with varying but mostly disappointing results,31⇓⇓⇓⇓-36 particularly for large and recurrent aneurysms.23
Stent Placement and Residual Aneurysms
The use of SAC, originally designed to treat otherwise untreatable aneurysms, has expanded in the hope of decreasing the risk of recurrences.3,6⇓-8,10⇓-12,37⇓⇓-40 This hypothesis has never been tested in a randomized trial. Previous studies,3⇓⇓⇓⇓⇓⇓-10 including systematic reviews and meta-analyses,11,12 have shown diverging results. Some studies have reported that aneurysms treated with SAC were less prone to recurrence,3,5,8,10⇓-12 while other studies did not show such an effect.4,6,7,9 Higher treatment-related risks of mortality and morbidity were shown in some reports,3,7,11 but not in others.4⇓-6,8,10 Many studies reported significant baseline differences between the groups being compared, most often with characteristics that could favor SAC (ie, a high proportion of unruptured sidewall aneurysms and shorter follow-up time).3⇓-5 Thus, after 20 years, we still lack reliable evidence regarding the risks and potential benefits of adding a stent to a coiling procedure in patients with UIAs eligible for both options. It is in this context of uncertainty that STAT was launched in 2011.
The Choice of Primary Outcome
The primary end point of STAT was a composite that included clinical and angiographic outcome measures. Although the main goal of UIA treatment is to prevent future ruptures, these are rare events.22⇓-24 Using death or disability from rupture during follow-up would necessitate the recruitment of thousands of patients followed for a long time. Most clinicians rely on angiographic results to assess the efficacy of treatment, and most endovascular trials have used angiographic outcomes as primary end points.22⇓-24 The residual aneurysm cutoff category was chosen to judge treatment failure because it has been shown to be more repeatable, and its clinical significance more constant than other categories.25 The clinical criteria included in the composite primary outcome measure ensured that a patient becoming dependent or dying because of a treatment-related complication (or because the treatment was clinically ineffective) would not count as a good outcome. However, clinical outcomes weighed little in the final comparison between treatments, which was driven mainly by angiographic results.
Primary Outcome Results
STAT did not show a large benefit of SAC over CA for the treatment of UIAs. This was true for patients with large (STAT-1), recurrent (STAT-2), or wide-neck aneurysms (STAT-3). The trial was only powered to show a large effect (a decrease in the failure rate from 33% to 15%). We cannot exclude that with the inclusion of a larger number of patients, a more modest but still clinically significant benefit could have been demonstrated.
In STAT, a substantial number of crossovers diluted the contrast between treatments. The classic way of analyzing results (intent to treat) remains clinically appropriate for practical reasons. First, many crossovers, such as bailout stent placement in patients with coil protrusion and parent vessel or branch occlusion (in the CA group) or failure to catheterize the branch necessary to land the stent (in the SAC group), were inevitable. Second, the goal of the trial was to assess the role of stent placement to intentionally improve the results of endovascular treatment. Perhaps the groups being compared could have been more precisely defined as SAC (if possible) versus CA plus bailout stent placement (only if necessary).
From an explanatory or mechanistic perspective, it is worth looking at the as-treated results: Does stent placement have the potential to improve the angiographic results of coiling?
Only by redefining a good angiographic outcome as a complete occlusion and only by looking at as-treated analyses could SAC be shown superior to CA (Online Supplemental Data). The clinical significance of this finding remains questionable, but it may be a signal in favor of the capacity of stent placement to improve angiographic results of coiling in the long term. This capacity may come at a cost in terms of complications: As-treated analyses also showed complications to be more frequent with SAC, particularly for small aneurysms. Although in some of these cases, complications occurred when stents were being used as a rescue strategy (ie, a technical complication had already occurred), thromboembolic complications with stent placement remain a concern.
Safety of Treatments
The overall morbidity and mortality of patients treated in STAT were within the range of our initial estimate (between 6% and 12%). Safety end points were similar between the 2 groups in intent-to-treat analyses, but the trial was underpowered to draw any conclusions about the safety of SAC over CA. The upper limit of the 95% CI of the risk ratio of 4.4 cannot exclude SAC being associated with a large increase in initial or long-term neurologic deficits compared with CA. Cerebrovascular ischemic and hemorrhagic events in STAT were relatively high compared with previous registries6,7 and meta-analysis.11 However, those comparisons are not valid, and aneurysms randomized in STAT were typically larger and many were difficult to treat by any and all methods.
Trial Limitations
Before we examine the potential impact on clinical practice, we must review the trial limitations. Only 4 centers participated, which limits the generalizability of results. Although STAT is the only randomized controlled trial comparing SAC and CA, the number of patients remains small. The introduction of flow diverters likely directed many patients with difficult aneurysms to other clinical trials.22 The original plan was to recruit 40–50 centers, but the lack of financial support deterred many potential centers from participating. As many as 600 patients would have been necessary to exclude the possibility that SAC would double the risk of death or dependency. Yet, safety is of primary importance when a preventive treatment is offered to mostly asymptomatic individuals. Many advanced SAC techniques, such as X or Y stent placement, were not frequently used, and trial results cannot be applied to these treatments. Most stents were braided stents (83%), and results may not apply to other types of stents. There were a substantial number of crossovers, diluting the contrast between groups in the intent-to-treat analyses. The 12-month follow-up period was relatively short. This may not have given enough time for some recurrences to become apparent. Clinical outcome assessments were not blinded, and core laboratory adjudications could not be masked to the presence of artifacts caused by stents. Death or dependency accounted for a relatively small number of poor outcomes in both groups (5-versus-6 patients, including 2-versus-3 deaths). Thus, potential bias from lack of blinding of mRS clinical assessors is unlikely to have significantly affected results. There were some disparities in follow-up imaging modalities between groups. However, because only residual aneurysms, readily identified by any imaging technique, were considered in the adjudication of the primary outcome, this potential bias is unlikely to have affected the results. Finally, the trial was conducted during 10 years. Indications, devices, techniques, and clinical expertise have evolved over such a long period.
Potential Implications for Practice and Future Research
STAT results do not apply to patients excluded by protocol, such as those with ruptured aneurysms. They do not apply to most small UIAs because only patients at high risk for recurrence (with large, wide-neck, or recurrent aneurysms) were eligible. Patients judged untreatable without stent placement, a subjective notion, were also excluded by definition.
For patients with UIAs treatable by both options, the trial showed no large benefit of a policy of stent placement in addition to coiling. In addition, the trial raises concerns regarding potential thromboembolic complications. This was particularly true for patients with small aneurysms at low risk of rupture, for whom the crucial question remains: Should they be offered preventive treatment at all?41
The use of stents for the treatment of UIAs is an example of the failure of our community to use randomized trials to safely introduce innovations in neurovascular care.2 We must find ways to integrate clinical research into practice to optimize care in real time.42 Future trials on SAC should probably be integrated into ongoing randomized clinical trials.41,43,44
CONCLUSIONS
STAT did not show SAC to be superior to CA for wide-neck, large, or recurrent unruptured aneurysms. More randomized data are needed to determine the role of SAC in the treatment of aneurysms.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 25, 2023.
- Accepted after revision February 16, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}