
Abstract
BACKGROUND AND PURPOSE: CSF leaks of the skull base and spine share a common process of CSF volume loss, and yet only the latter has been associated with spontaneous intracranial hypotension (SIH). Despite published claims that only spinal leaks cause SIH, no prior studies have evaluated brain MR imaging in patients with skull base leaks for findings associated with SIH, such as dural enhancement. The purpose of our study was to use a validated brain MR imaging scoring system to evaluate patients with skull base CSF leaks for findings associated with SIH.
MATERIALS AND METHODS: We included patients with confirmed skull base CSF leaks and contrast-enhanced preoperative brain MRI. The preoperative MR images were reviewed for findings associated with SIH by using the Bern score. Patient age, presenting symptoms and their duration, and leak site were also recorded.
RESULTS: Thirty-one patients with skull base CSF leaks were included. Mean Bern score was 0.9 (range 0–4, standard deviation 1.1), and only 1 patient (3%) had dural enhancement. Mean age was 53 years (range 18–76). Mean symptom duration was 1.3 years, with 22 patients presenting within 1 year of symptom onset. Twenty-three patients (74.2%) had intraoperative confirmation of leak from the middle cranial fossa, involving the temporal bone, while 7 (22.6%) had leaks from the anterior skull base. One patient, who had dural enhancement, had an infratentorial CSF leak along the petrous segment of the internal carotid artery.
CONCLUSIONS: Our study provides further evidence that skull base and spinal CSF leaks represent distinct pathophysiologies and present with different brain MRI findings.
ABBREVIATIONS:
- IIH
- idiopathic intracranial hypertension
- SIH
- spontaneous intracranial hypotension
SUMMARY SECTION
PREVIOUS LITERATURE:
Prior studies have described that spinal CSF leaks cause spontaneous intracranial hypotension (SIH), but that skull base CSF leaks do not. This is based on the absence of skull base CSF leaks in a cohort of patients with SIH, but without direct study of skull base CSF leaks.
KEY FINDINGS:
We specifically studied patients with skull base CSF leaks and found that they do not have brain MR imaging findings that are associated with SIH.
KNOWLEDGE ADVANCEMENT:
Our study adds to the body of literature advocating that SIH is caused by spinal CSF leaks but not skull base CSF leaks.
Spontaneous intracranial hypotension (SIH), caused by a CSF leak, can present with debilitating symptoms, including orthostatic headache, dizziness, and even dementia-range neuropsychiatric changes or coma.1 As the name implies, SIH was initially thought to be due to low intracranial CSF pressure.2 Since that time, however, other publications have shown that most patients with SIH have normal CSF pressure, and thus the underlying etiology has been attributed to low CSF volume.3 Per this mechanism, any site of CSF loss with subsequent low CSF volume might be expected to lead to the same disorder. Abnormal brain MR imaging findings can be explained based on the Monro-Kellie doctrine,4 in that the loss of CSF is replaced by venous blood with resultant dural enhancement, venous engorgement, subdural fluid collections, and venous engorgement of the pituitary. Spontaneous skull base CSF leaks, frequently associated with intracranial hypertension and often present with CSF leakage through the nose or ear, should therefore have overlapping sequelae as spinal CSF leaks. The contrary has been described, predominantly based on a study by Schievink et al5 that reviewed a collection of patients with SIH, none of whom were found to have a skull base CSF leak. The dissociation of skull base leaks from the clinical symptoms and brain MRI findings of SIH has been propagated in the literature despite the absence of prior studies specifically evaluating skull base CSF leaks.6,7 The purpose of the current study was to evaluate patients with skull base CSF leak for SIH clinical symptoms and brain MRI findings by using a validated scoring system.
MATERIALS AND METHODS
We reviewed a historical database of patients with skull base CSF leaks seen at our referral center from 2009–2017. Individual patients were reviewed and included if they had a confirmed skull base CSF leak and preoperative contrast-enhanced brain MRI. Each brain MRI was reviewed for cerebellar tonsil descent below the foramen magnum and Bern score components8 (Table 1), which include dural enhancement, small suprasellar cistern (≤4 mm), and venous engorgement (2 points each), as well as for a small prepontine distance (≤5 mm), small mamillopontine distance (≤6.5 mm), and subdural fluid collections (1 point each). Electronic medical records were reviewed for age, symptoms and their duration, location of CSF leak, history associated with CSF leak, and lumbar puncture with opening pressure. Descriptive statistical analysis, including mean, SD, and range, were reported.
Bern score criteria and scoring system
RESULTS
Thirty-one patients (mean age 53 years, range 18–76) with skull base CSF leaks and preoperative contrast-enhanced brain MRI were identified and included in this study (Fig 1). All cases had intraoperative confirmation of a skull base CSF leak. Eight patients (25.8%) presented with headaches: 1 was constantly orthostatic, 3 were intermittently orthostatic, 1 overlapped with diagnosed infectious meningitis, 1 was worse when supine, and 2 were not further characterized. Excluding the patient with meningitis, no patients reported photophobia, phonophobia, or cognitive issues. Eighteen patients presented with otorrhea, 8 with rhinorrhea, and 5 had neither otorrhea nor rhinorrhea but had brain MRI findings of a meningoencephalocele and an intraoperative dural defect. The mean symptom duration was 1.3 years, with 22 patients presenting within 1 year of symptom onset.

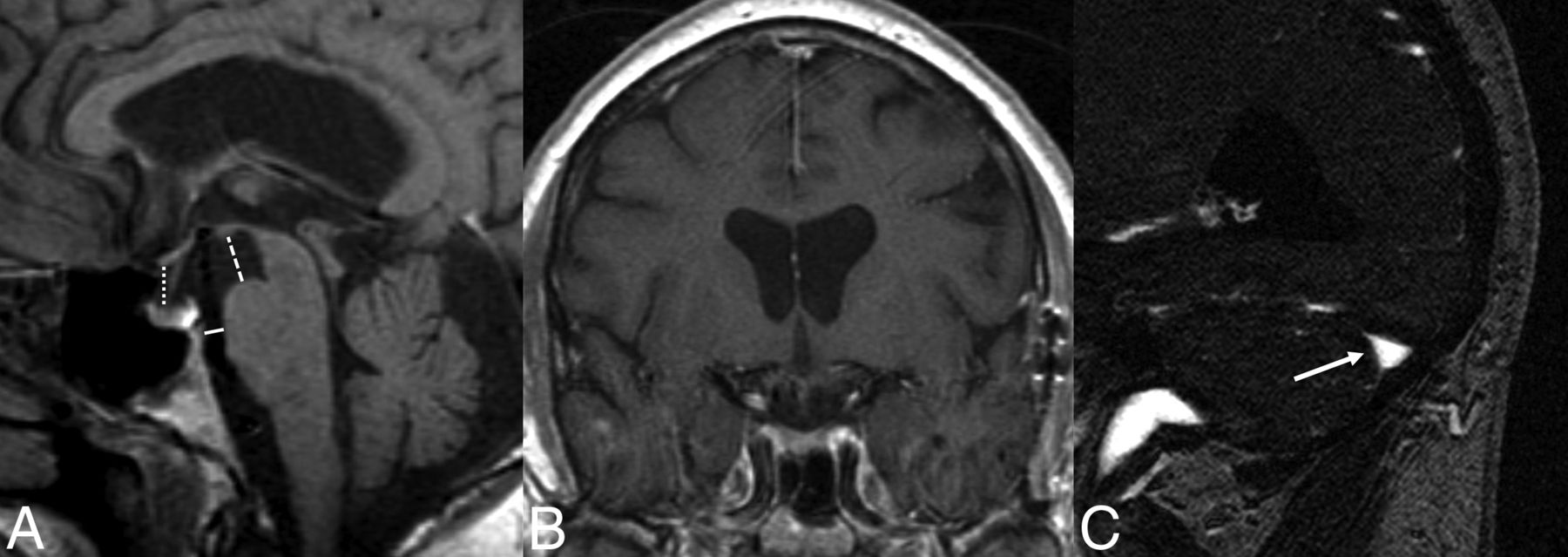
A 57-year-old man with a surgically proved right tegmen tympani CSF leak without brain MR imaging findings associated with SIH (Bern score = 0). A, Sagittal T1-weighted image shows normal suprasellar (dotted line), mamillopontine (broken line), and prepontine distances (solid line). B, Contrast-enhanced coronal T1-weighted image shows normal dura without thickening or enhancement. C, Sagittal image from an MRV shows a nondistended dominant transverse sinus (arrow).
Most patients (23/31, 74.2%) had intraoperative CSF leaks found in the middle cranial fossa involving the temporal bone. Seven (22.6%) had an intraoperative CSF leak found in the anterior skull base. One patient (3.2%) had infratentorial CSF leaking along the petrous portion of the internal carotid artery and had orthostatic headache. For medical history relevant to the skull base CSF leaks, 3 patients (9.7%) had the diagnosis of idiopathic intracranial hypertension (IIH), 6 (19.4%) had a history of trauma, 9 (29.0%) had prior temporal bone surgery, and 13 (41.9%) were spontaneous.
The mean Bern score was 0.9 (range 0–4, SD 1.1). Lower Bern scores are associated with lower likelihood of finding a spine CSF leak or CSF-venous fistula on subsequent myelography (score 0–2 low and 3–4 intermediate likelihood) (Table 2).8,9 Brain MRI findings are summarized in Table 3. Only 2 patients had a Bern score higher than 2, 1 patient with headache and an infratentorial leak (Bern 4, dural enhancement and venous distension), and 1 patient whose brain MRI findings (Bern 4, small suprasellar, prepontine, and mamillopontine intervals) without headache were unchanged 1 year after CSF leak repair.
Interpretation of total Bern Score
Brain MRI findings in patients with skull base CSF leaks
DISCUSSION
Our study used a validated brain MRI scoring system to assess for SIH in patients with skull base CSF leaks. Previously, skull base CSF leaks have been seen as distinct from SIH based on a single study that evaluated patients with SIH and did not find any with skull base CSF leaks. Patients with skull base CSF leaks have not previously been studied for brain MRI findings of SIH. Of the 31 patients included in our study, the mean Bern score was less than 1, and only 1 patient had dural enhancement. Only 4 had headaches with orthostatic features. Our findings provide further evidence of the distinct underlying pathophysiology of skull base and spinal CSF leaks.
The initial work from Dobrocky et al8 described a probabilistic brain MRI scoring method (0–9, 9 representing the highest probability) to measure the likelihood of a spinal CSF leak, frequently referred to as the Bern score, and reported an 83% rate of dural thickening/enhancement in patients with SIH. Subsequent studies have described a similar rate of dural enhancement in SIH of 79%10 and 81%.11 Our study population largely did not demonstrate findings of SIH, with a mean Bern score of less than 1 and only 1 case (3%) with dural enhancement. Kranz et al12 found that increasing symptom duration is associated with decreased rate of dural enhancement and that patients with SIH without dural enhancement had a mean symptom duration of 45.3 weeks. In our study, 22 patients had symptom duration of 1 year or less (1 had dural enhancement), including 10 with symptom duration of 6 months or less (none had dural enhancement).
The major prior study that separated skull base CSF leaks from spinal CSF leaks causing SIH was performed by Schievink et al,5 who reviewed 273 patients with SIH from a single institution and did not find any cases with a skull base CSF leak. Schievink et al13 later reported a single case of SIH caused by a skull base leak from the posterior fossa. Tai et al14 reported on the treatment and outcomes in patients with spontaneous versus nonspontaneous CSF leaks, and included 6 patients with spontaneous sphenoid sinus leaks. They stated that all 6 patients had MRI findings of intracranial hypotension, but did not use a validated scoring system for MRI results, nor did they list what imaging findings were abnormal. Their methodology included focal dural enhancement as a sign of SIH, which in a different study has been described as an SIH mimicker,15 and is likely distinct from the diffuse dural enhancement that is widely associated with SIH. Our study evaluated the MR imaging findings in skull base CSF leaks by using a validated scoring system and did not find brain MR imaging results associated with SIH.
Spinal and skull base CSF leaks both result in CSF loss, but they are differentiated by the leak location. Why would the location of the CSF leak cause such different symptoms and brain imaging findings? It is likely that brain MRI in SIH is related to downward CSF shift in the cranial-to-caudal direction from a sump effect of the spinal CSF leak. Wolf et al16 recently used phase-contrast MRI in patients with SIH (spinal leaks) to show that CSF flow was increased at C2–C3 compared with normal controls. They also found that patients with SIH had larger craniocaudal spinal cord motion at C2–C3. Comparatively, in our study, skull base CSF leaks would theoretically have preserved physiologic CSF flow at the skull base, without resultant downward sump effect that would cause brain sag or venous engorgement (Fig 2).

Illustration of a patient with a spontaneous supratentorial skull base CSF leak in the middle cranial fossa (A) with preserved CSF flow at the foramen magnum (B). This is in contrast to a patient with a spinal CSF leak (C) that could include a ventral dural tear or CSF-venous fistula, and potential sump effect with craniocaudal CSF flow at the foramen magnum (D) that contributes to findings associated with SIH including brain sag and pituitary engorgement shown here.
Most interesting, the 1 patients with skull base CSF leaks in our cohort with dural enhancement had an infratentorial CSF leak. Before surgical repair of the skull base CSF leak, the patient underwent a conventional CT myelogram that did now show extradural fluid. Three years later, the patient was found to have a ventral spinal CSF leak from a calcified disk osteophyte complex. It is unknown whether the patient’s symptoms were due to an occult spinal CSF leak or if this occurred after the skull base leak repair. All other patients in this study without dural enhancement had supratentorial CSF leaks, suggesting that supra- versus infratentorial leak location could contribute to the brain MRI findings. One prior case report described a cranial CSF leak presenting with orthostatic headache and brain MRI findings that included diffuse dural enhancement, and this patient also had a posterior fossa CSF leak into the mastoid air cells.17 Bonomo et al18 reported a single case of a small spheno-ethmoidal meningoencephalocele causing SIH symptoms and brain MRI findings, but no other studies have described similar findings. Therefore, the notion that SIH is caused by a spinal CSF leak might possibly be extended to leaks from the infratentorial skull base, however the current data are insufficient to fully support this claim.
Our study has limitations, starting with the retrospective nature and small sample size. Spontaneous skull base leaks are rare, but to our knowledge, we present the largest study focusing on brain MRI findings. Our theory, building on what Wolf et al16 reported in patients with SIH, requires testing. Further studies evaluating upper cervical CSF flow and cord motion in skull base CSF leaks could help to validate our hypothesis. Nonetheless, it has been suggested that skull base CSF leaks do not present with SIH, and our study largely supports this claim. One of the 2 patients with an intermediate Bern score of 4 in our study had brain sag and low-lying cerebellar tonsils that were unchanged 1 year after surgical repair of the CSF leak. The lack of improvement of the brain MRI findings, if the causative leak site was repaired, would be unexpected based on prior work by Dobrocky et al19 studying postoperative brain MRI findings in patients with surgically repaired spinal CSF leaks. It is possible that our patient’s findings represented a Chiari type I malformation rather than sequela of a CSF leak. Additionally, outside of the infratentorial CSF leak, none of the patients with headache in our study were evaluated for a spinal CSF leak, and therefore a spinal cause was not excluded.
CONCLUSIONS
Prior studies have suggested that skull base CSF leaks, as opposed to spinal CSF leaks, do not present with SIH. This idea was largely based on observations of spinal CSF leaks only. We approached the question from the perspective of skull base CSF leaks and found further evidence for the same conclusion. Skull base leaks and spinal CSF leaks may indeed represent distinct disorders of CSF dynamics.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received March 29, 2024.
- Accepted after revision May 1, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}