
SUMMARY:
This study assesses the efficacy of low-field portable MR imaging in measuring ventricular volumes in the pediatric population in the hospital setting. We compared portable and standard of care MR images from the same patient. The estimated ventricular volumes had excellent agreement with a mean bias of 2.06% by Bland-Altman analysis and a correlation of 0.99. From this initial data set, our results suggest that low-field, portable MR imaging is a promising technique for imaging and quantifying ventricular volumes.
ABBREVIATIONS:
- CMKC
- Children’s Mercy Kansas City
- SOC
- standard of care
Increased intracranial ventricular volumes in infants are associated with many neurologic diseases. Increased ventricular volumes can be seen in the setting of posthemorrhage hydrocephalus, congenital hydrocephalus such as cerebral aqueductal stenosis, and decreased brain volume due to prematurity or other neonatal insults.1,2 Increased intracranial ventricular volumes at birth are associated with impaired neurodevelopmental and motor and language function at 2 years.3 Therefore, tracking changes in ventricular size and shape can be helpful in caring for infants.
Hyperfine has developed a portable low-field MR imaging device with a magnetic field strength of 64 mT. The reduced magnetic field strength moderates safety concerns and allows imaging at the bedside. This portability eliminates the need for a separate MR imaging suite and patient transport.4,5 Sien et al6 recently demonstrated and described the safe use of portable MR imaging in the pediatric intensive care unit setting. However, the trade-off is that the portable MR imaging sequences often have lower spatial resolution and/or lower signal to noise than conventional MR imaging for the same scan time.7
Given the unique advantages of the low-field portable MR imaging, we wanted to assess its effectiveness in measuring ventricular volumes in the pediatric population. We hypothesized that ventricular volumes estimated by low-field, portable MR imaging scans would be comparable with conventional MR imaging estimates.
MATERIALS AND METHODS
Patient Cohort and Inclusion and Exclusion Criteria
We conducted a retrospective analysis of data acquired as a part of a prospective cohort study of patients who had portable MR images obtained in the Neonatal Intensive Care Unit and Pediatric Intensive Care Unit at the Pediatric Intensive Care Unit at Children’s Mercy Kansas City (CMKC) from November 2020 to August 2022. This study was approved by the CMKC institutional review board, and informed parent consent was obtained for all study participants. For the prospective study, patients undergoing a conventional MR imaging and younger than 22 years of age at CMKC were eligible. Parents were approached for informed consent, and if consent was obtained, then the patients were included. Patients who weighed <2 kg or were deemed unlikely to be able to remain still for 1 hour were excluded. No sedation was used for either portable or standard of care (SOC) MR imaging. Due to the limited time window, limited study resources, parent availability, and patient acuity, consent and enrollment have been much more common in our Neonatal Intensive Care patient population. From the prospective data set, we included patients who underwent low-field MR imaging using portable MR imaging either at their bedsides or in the department of radiology and had a conventional brain MR imaging within 24 hours of the portable MR imaging examination.
Patient Cohort
Seventeen patients had both SOC and portable MR imaging scans during the date range of our study, as described in Table 1. The most common indications for the SOC MR imaging were trauma (n = 4), altered mental status (n = 3), hemorrhage (n = 2), and stroke (n = 2). The other indications are listed in Table 1. No patients were excluded. The age of patients ranged from 4 days to 83 days, with a median age of 7.5 days, and mean age of 22 days. Although most patients were neonates, there were 2 patients older than 60 days of age.
MR Imaging Scans
SOC T2-weighted, axial MR images acquired at either 1.5T or 3T (Magnetom Avanto Fit or Magnetom Prisma; Siemens) were used as a reference comparison for ventricle volume assessment. The SOC TSE (n = 16) and HASTE (n = 1) scans were acquired with the parameters listed in Table 2. Portable MR images used for ventricle volume estimation included T2-weighted spin-echo sequences (n = 17). Parameters for the portable MR images are also listed in Table 2. The portable MR images were acquired with the Hyperfine Swoop software Versions 8.1 to 8.5. Two reconstruction algorithms were used for portable MR images (standard reconstruction = 7/17, deep learning reconstruction = 10/17).
| Participants | |||
|---|---|---|---|
| No. | % | ||
| Biologic sex (at birth) | |||
| Female | 7 | 42 | |
| Male | 10 | 58 | |
| Ethnicity | |||
| White | 11 | 65 | |
| African American | 1 | 6 | |
| Asian | 2 | 12 | |
| Other | 3 | 18 | |
| Indication | |||
| Trauma | 4 | 24 | |
| Altered mental status | 3 | 18 | |
| Hemorrhage | 2 | 12 | |
| Ischemic stroke | 2 | 12 | |
| Infection | 1 | 6 | |
| Hydrocephalus | 0 | 0 | |
| Lesion/mass | 0 | 0 | |
| Mean time to acquire images (min) | |||
| SOC | 23 (SD, 14) | ||
| Low-field | 32 (SD, 13) | ||
| Age (days) | 22 (SD, 7) | ||
General demographics of the study population, including indications for MR imaging that may influence ventricular volumes
Segmentation
The software used for segmentation was ITK-SNAP (Version 3.8.0; www.itksnap.org),8 which allowed simultaneous viewing of the ventricles in all 3 orientations. T2-weighted axial images were used for visualizing the lateral, third, and fourth ventricles, which were segmented by a medical student (V.V.) and verified by a pediatric radiologist with 8 years of experience in pediatric neuroradiology (S.S.C.). Due to the difference in image quality, it was not possible to blind the reviewer to the type of image. However, the review order was randomized, and studies were performed 1 study at a time, so the reviewers were blinded to the volumes measured on other images including the patient’s matched imaging. The segmentation time depended on the complexity and image resolution of the individual and averaged 20 minutes per patient. Proper identification of the ventricles was confirmed by the signal intensity of the CSF in the ventricles compared with normal brain parenchyma. For each image segment, the freehand paintbrush tool (a manual segmentation technique) was used to outline the lateral, third, and fourth ventricles to calculate voxel counts. The ventricular volumes were then calculated by multiplication of the number of voxels by the voxel volume.
Statistical Tests
Statistical analysis of the data was performed using SPSS Statistics (Version 27; IBM). Descriptive statistics were reported using mean (SD) and median (range). Bland-Altman9 analysis and correlations were used to compare the SOC and portable MR imaging volumes.
RESULTS
MR Images and Segmentation
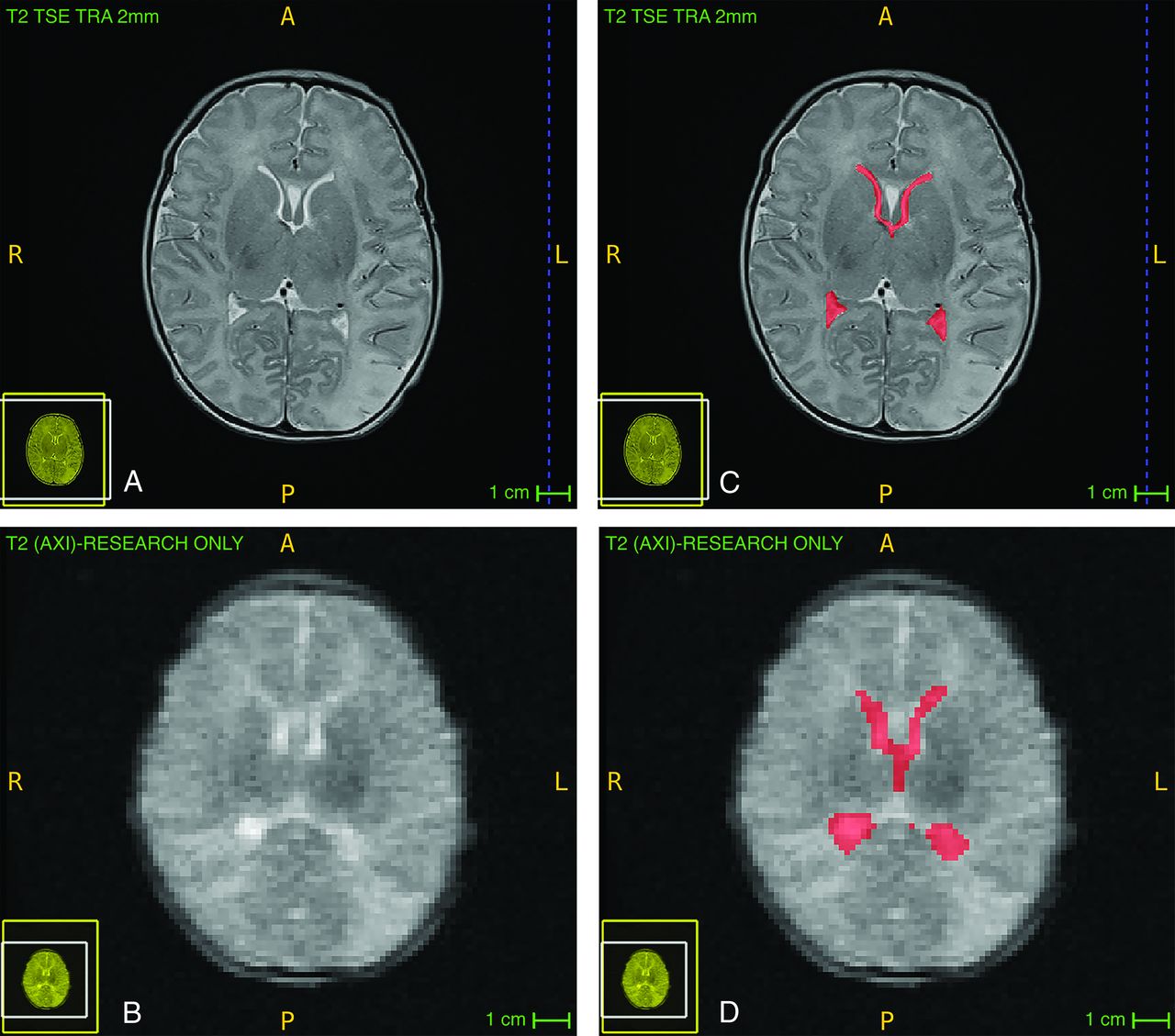
Figure 1 shows conventional and portable MR images in the same patient along with the manual segmentation performed. The median ventricular volumes (portable MR imaging, median [range high-low] 12.66 [55.0–6.6] cm3; SOC 12.4 [54.2–6.2] cm3) were similar, with a slight increase in the volume estimate for portable MR imaging. The correlation coefficient was very high (r2 = 0.9993) between portable MR imaging and conventional MR imaging (Fig 2).

Comparison of SOC and portable clinical MR imaging as well as examples of manual segmentation in 1 participant, a 4-day-old boy without intracranial abnormalities such as ischemia or hemorrhage. Segmentation at 1 level of the lateral ventricles is shown here; SOC (A), SOC with segmentation (B), portable (C), portable with segmentation (D). Hyperfine scans were acquired with software, Version 8.1.0.1. TRA indicates transaxial; AXI, axial; R, right; L, left; P, posterior; A, anterior.

Portable MR imaging versus SOC MR imaging–estimated ventricular volumes. The ventricular volumes using Hyperfine and SOC MR images are plotted. The ventricular volumes of each set of images for the 17 patients were estimated using ITK-SNAP.
Bland-Altman Analysis
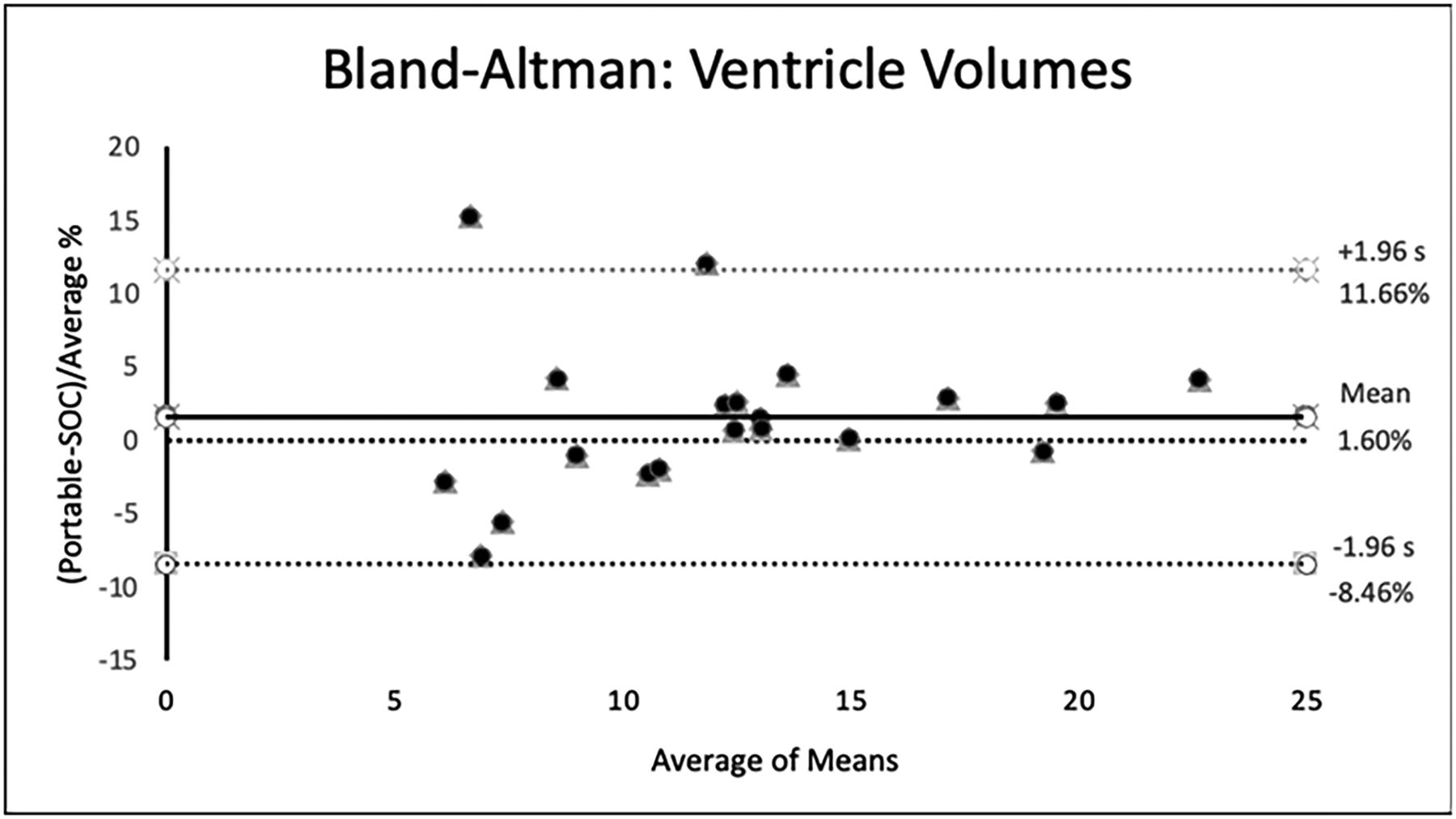
In this study, we selected a priori limits of the maximum acceptable difference of 15% based on biologically and analytically relevant criteria.10 The Bland-Altman analysis (Fig 3) suggested no substantial bias, because the line of equality was within the confidence interval.9 The mean bias was 2.06%, indicating increased volume estimated with portable MR imaging. The agreement limits were −8.64%–12.78%. The range of agreements lay within our desired reference range of 15%, even with the small sample size of 17. Because neither of the limits were exceeded, the measurements obtained from portable MR imaging provide an acceptable estimate compared with SOC MR imaging in this patient population.

Results of the Bland-Altman analysis. Plot of differences between method A (portable) and method B (SOC), expressed as percentages of the values on the axis [(portable – SOC) / mean%)], versus the mean of the 2 measurements. The bias (mean difference) of 2.06% is constant, with greater variation for lower ventricular volumes. s indicates standard deviation.
DISCUSSION
We showed high correlation and no systemic bias in the estimates of ventricular volume using low-field, portable MR imaging compared with SOC MR imaging in infants. From this initial data set, our results suggest that low-field, portable MR imaging is a promising technique for imaging and quantifying ventricular volumes.
The results of our study are clinically relevant because ventricular volume measurements are clinically useful to guide management. This result is especially important in the setting of hydrocephalus when repeat measures across time are useful but can be burdensome to the patient and health care team. Hydrocephalus is currently imaged with head CT and rapid-sequence brain MR imaging, which consist of limited T2 sequences. However, there are distinct disadvantages to rapid-sequence brain MR imaging: The reduced number of sequences reduces the sensitivity and diagnostic accuracy.11 The prior conceptions of low-field MR imaging included the intraoperative Polestar −10 iMRI system (Odin Medical Technologies) approved in 2002.12 Limitations include strict patient positioning, the inability to perform specialized imaging protocols such as DWI or FLAIR, and impaired clinical utility outside the operating room.13 The Hyperfine Swoop portable MRI scanner has the ability to supplement these imaging techniques because it combines easier access similar to CT with the nonionizing radiation advantage of MR imaging. Portable MR imaging could even be more accessible than CT because it could be located at bedside or in the clinic.14
Study limitations include the small sample size and being performed at a single site. Also, no patients with shunted hydrocephalus were in this cohort, though there were patients with enlarged ventricles. While the lack of patients with hydrocephalus and a narrow age range were limitations, the high agreement within a relatively narrow range of ventricle volumes for most patients makes it highly likely that larger pathologic volumes could be reliably detected. Another limitation was possible bias in segmentation because there was no way to blind the segmentation process to the type of scan because of the visible difference in scan resolution. However, we blinded the person performing the segmentation to the volume results of the corresponding images.
Larger studies in the hydrocephalus patient population would be useful for validation. Currently, there is some image distortion from portable scanner images, so it can be challenging to segment the ventricular volumes. However, manual segmentation can be implemented with high reliability and accuracy when performed properly, but it is labor-intensive.15 Fully or semiautomatic segmentation is possible, but the current automatic segmentation methods (eg, FreeSurfer) struggle with lower-resolution images.15 In the future, we expect further optimization of image-acquisition methods and pulse sequences that will allow more accurate analysis.15
CONCLUSIONS
When compared with SOC MR imaging, low-field, portable MR imaging estimates of ventricular volume had excellent agreement with ventricular volumes measured by conventional MR imaging.
Scan parameters for SOC and Hyperfine scans used for ventricle volume quantification
Acknowledgments
We thank the Medical Writing Center at CMKC and Dr Avner Meoded for editing this manuscript.
Footnotes
↵# Adam Rouse and Sherwin S. Chan are co-senior authors.
This work was supported by an investigator-initiated grant from Hyperfine Inc to Sherwin S. Chan at Children’s Mercy, Kansas City.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 22, 2024.
- Accepted after revision February 23, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.