
SUMMARY:
Vagus nerve stimulation devices are conditionally approved for MR imaging with stimulation turned off, and the requirement to modify the stimulation settings may be a barrier to scanning in some radiology practices. There is increasing interest in studying the effects of stimulation during MR imaging/fMRI. This study evaluated the safety of standard and investigational microburst vagus nerve stimulation therapies during MR imaging/fMRI. A prospective, multicenter study was conducted in patients with an investigational vagus nerve stimulation device that delivered either standard or investigational microburst vagus nerve stimulation. Thirty participants underwent sequential MR imaging and fMRI scans, encompassing 188 total hours of scan time (62.7 hours with standard vagus nerve stimulation and 125.3 hours with investigational microburst vagus nerve stimulation). No adverse events were reported with active stimulation during MR imaging or during 12 months of follow-up. Our results support the safety of standard and investigational microburst vagus nerve stimulation therapy during MR imaging and fMRI scans.
ABBREVIATIONS:
- DRE
- drug-resistant epilepsy
- FOS
- focal-onset seizures
- µVNS
- microburst VNS
- PGTC
- primary generalized tonic-clonic seizures
- VNS
- vagus nerve stimulation
Approximately one-third of patients with epilepsy will develop drug-resistance and may be candidates for alternative therapies, including neuromodulation.1 In 1997, the FDA approved the use of vagus nerve stimulation (VNS) as an adjunctive therapy for decreasing the incidence of focal-onset seizures (FOS) resistant to antiepileptic medications in adults and adolescents older than 12 years.2
VNS devices are surgically implanted under the skin in the upper chest area and connected to the left cervical vagus nerve (Fig 1). Standard VNS sends tonic pulse trains of stimulation (eg, 1-, 2-, or 5–30 Hz signal frequency in 5 -Hz increments) to the brain through the vagus nerve to treat seizures.3 Pulse delivery to cortical areas is believed to be mediated by nuclei close to the brainstem. There has been increasing interest in investigational microburst VNS (µVNS) consisting of high-frequency bursts (eg, 100–350 Hz signal frequency in 50-Hz increments in small pulse trains of 4–7 pulses/burst), which has preclinical evidence to suggest that it works by modulating other areas of the brain, including the thalamus.4,5

Implanted VNS device. The pulse generator is implanted in the left chest, and the lead is connected to the left vagus nerve in the neck. VNS pulses are delivered to the brain via the vagus nerve. Adapted with permission from Verner et al.3
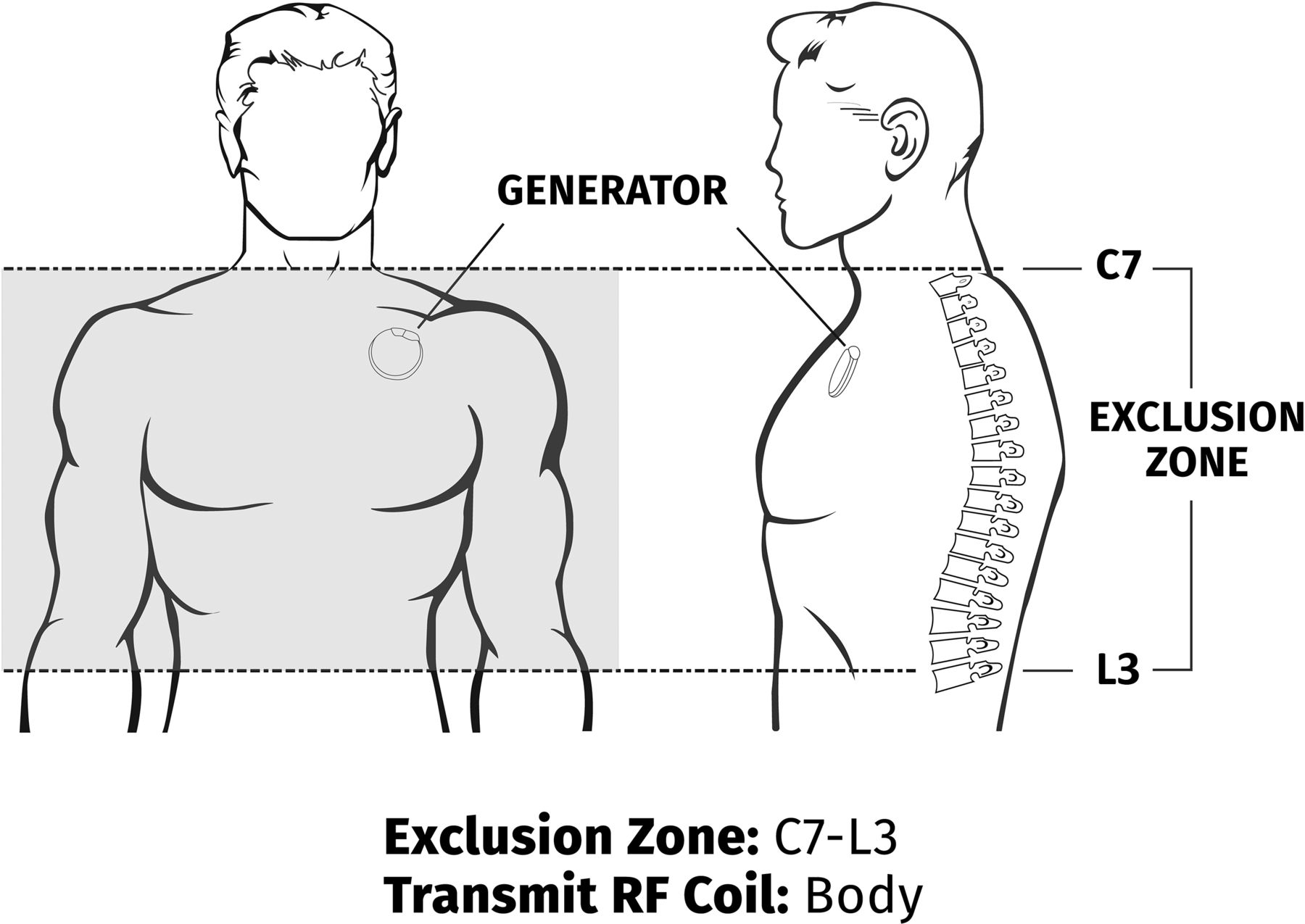
These implants are encountered frequently in patients needing MR imaging. FDA-approved standard VNS therapy has instructions that recommend turning the stimulation current off to safely scan patients. VNS pulse generators are designed with a magnetic reed switch intended to either inhibit stimulation (in the presence of a suitable magnetic field) or trigger on demand stimulation after a brief exposure to the magnetic field. fMRI has been performed safely and effectively with previous commercially-approved models of the pulse generator with careful orientation of the device (the strong B0 field does not interact with the reed switch).6 Current VNS devices carry an MR conditional rating at 1.5T and 3T by the FDA, and MR imaging can be safely performed under the specified conditions with a body coil or a local transmit/receive coil (Figs 2 and 3).7 The approved conditions require modified device programming during MR imaging to turn the stimulation current off, and MR imaging facilities may lack staff familiar with adjusting the device settings to comply with these conditions.7 This article reports safety results from a prospective trial of patients undergoing 3T MR imaging and fMRI during the administration of standard VNS and investigational µVNS therapy. The feasibility protocol is published elsewhere.3

Exclusion zone and permissible area during MR imaging for the head and extremity using local transmit/receive head or extremity coils. RF indicates radiofrequency.

Exclusion zone and permissible area during MR imaging for the body using the body-transmit coil and the local receive-only coil.
MATERIALS AND METHODS
This prospective, interventional, unblinded multicenter study (NCT03446664) designed to collect data from patients with drug-resistant epilepsy (DRE) 12 years of age and older with an implanted investigational VNS (Model 1000C µB SenTiva VNS Therapy System; LivaNova USA) was conducted between February 1, 2018, and October 7, 2021.8 The study was in accordance with the ethical principles of the Declaration of Helsinki consistent with Good Clinical Practice described in ISO 14155 (https://en.wikipedia.org/wiki/ISO_14155) and the applicable regulatory requirements. All study participants provided informed consent, and study sites adhered to the institutional review board/ethics committee (https://clinicaltrials.gov/study/NCT03446664).
The investigational VNS device, Model 1000C, is physically identical to the conditionally approved Model 1000 (SenTiva VNS Therapy System) except for markings and firmware changes (Online Supplemental Data). Testing for the Model 1000 followed the requirements of ISO 14708–3, which indicates ISO/TS 10974 as the proper methodology for MR conditional assessments of active implantable medical devices. Modifications of the Model 1000 for the investigational Model 1000C included configuration to deliver either commercially available standard VNS or investigational µVNS. The investigational VNS device is also configured with the ability to disregard the reed switch response under the presence of a magnetic field, removing the necessity for any careful alignment with respect to the B0 field. Additional testing was performed on the Model 1000C, the investigational VNS device, to monitor stimulation output during MR imaging (normally off) and was submitted as part of the investigational device exemption submission. No additional MR imaging device interaction risk was created by adding the stimulation output.
We studied 2 groups: 1) those with FOS and, 2) those with electroencephalogram-verified primary generalized tonic-clonic seizures (PGTC). Participants were neuromodulation-naïve, and additional investigational devices and/or investigational drugs were not permitted.
Participants underwent sequential fMRI at 2 weeks and 1-, 3-, and 6-month visits.3 They were placed in the 3T MR imaging scanner and had a series of 3 fMRI scans per visit with VNS “on” and a minimum scan time of 30 minutes (6 levels, 5 minutes per level) per day. There was an additional scanning time with the VNS “off,” which could add 10–15 minutes per session, which included structural MR imaging and resting-state fMRI. The time for patient positioning in the magnet varied with an additional 5–10 minutes per session. Participants were instructed to inform the physician, radiologist, and/or MR imaging technologist overseeing the procedure if they experienced any adverse effects during their scans. Inquiries were also made by the study investigator of the participant during each visit.
A single-channel transmit/receive head coil was used for data-acquisition. Recent regulatory approval under “group A” scan conditions permits the use of the body-transmit coil. However, those parameters are more stringent than the transmit/receive head coil, and using the body coil would have necessitated modifications to the proposed study protocol versus the initial pilot study. Each scan included acquisition of a localizer scan and an isotropic 3D T1-weighted anatomic sequence followed by fMRI during active stimulation of the VNS device (either standard or microburst).3 Functional data were acquired using gradient-echo EPI with the following parameters: TR/TE = 3000/25 ms, flip angle = 84°, voxel size = 3 mm isotropic, FOV = 256 mm, whole-brain coverage, 603 measurements, and a partial Fourier factor = 6/8. fMRI scans were obtained in a dose-dependent manner, leveraging a block design with 30 seconds of stimulation (on time) followed by 30 seconds of no stimulation (off time). Each on/off cycle was repeated 5 times for a total of 5 minutes before the parameter was changed for the next 5 minutes. Six 5-minute cycles were used for the fMRI scanning time of 30 minutes. During the fMRI study procedures, the parameter sweep feature on the investigational device was used and the reed switch (used to either inhibit or stimulate in Magnet mode) was disregarded.3
The study design required participants to have the device stimulated during the parameter sweep phase while undergoing the fMRI, so the fMRI results could further guide therapeutic adjustments. Following completion of a parameter sweep, the reed switch response was re-enabled and functioned as intended for normal use of the stimulator. Participants were continuously monitored by the MR imaging technologist and the LivaNova (device manufacturer) field engineers during and between scans.
Statistical analysis was not conducted to compare the demographics or outcomes of the study groups; therefore, no formal sample size calculation was provided.8 The number of subjects per cohort was deemed sufficient to provide initial information on the safety of the device. The final analysis was conducted when all participants completed the study at month 12.
RESULTS
A total of 33 participants (n = 21 FOS and n = 12 PGTC seizures) were enrolled, of whom 32 (n = 20 FOS and n = 12 PGTC seizures) were implanted with the investigational µVNS device. One participant was lost to follow-up before implantation of the device. Within the group of participants with implanted devices, 30 participants (n = 19 FOS and n = 11 PGTC seizures) completed the study (Fig 4). Within the implanted study population, one-half were men (n = 16; 50%) and one-half were women (n = 16; 50%), and the sexes were also equally represented in both cohorts. Most of the subjects were white (n = 29; 90.6%) and not Hispanic or Latino (n = 30; 93.8%). The mean age was 31.2 (SD , 13.7) years (range = 14–61 years).

Microburst participant accountability showing the initial enrollment through study completion plus study attrition.
Following implantation and a 2-week recovery, participants reported to the research site and the MR imaging scanning facility to have their VNS device turned on and titrated following an fMRI assessment. Three additional titrations without fMRIs were completed between the 1- and 3-month fMRI visits to help the participants acclimate to the increases in the output current for microburst stimulation. The participants also underwent a VNS tolerability paradigm test in which the maximum tolerable output current was determined for standard VNS and µVNS. The VNS parameter settings at the start of each follow-up visit are listed in the Online Supplemental Data. On completion of the third fMRI scan at each visit, the VNS device was programmed to the microburst settings, resulting in the greatest thalamic activation (ie, spatial extent and peak intensity). Participants continued to report to the site for safety follow-up visits at 9 and 12 months.
There were no reported adverse events from the participants during active fMRI with the investigational VNS device in the 188 hours of active scan time (62.7 hours with standard VNS stimulation and 125.3 with investigational microburst VNS stimulation). There were also no issues with image quality.
DISCUSSION
VNS therapy is a less invasive, peripheral approach to alter epileptic networks that has been proved safe and effective for a variety of seizure types. Commercially-approved standard VNS and investigational µVNS devices are MR conditional. The investigational µVNS device used in this study was designed and approved to be capable of delivering standard and investigational µVNS therapy while inside the MR imaging scanner and is subject to scanning requirements of commercial devices.
Knowledge of the commercial and investigational VNS devices, the current conditional guidelines for standard VNS (low frequency, ≤30 Hz) therapy with MR imaging, and the investigational µVNS (high frequency, 250–350 Hz) therapy can help assuage the concerns of radiologists and MR imaging technologists. A thorough understanding of the 3 available modes of therapy (eg, Normal, Magnet, and AutoStim) with the investigational µVNS and its MR imaging–compatible design for 1.5T and 3T is essential. The investigational µVNS devices used in participants scanned for 188 hours (62.7 hours with standard VNS stimulation and 125.3 with investigational microburst VNS stimulation) with no adverse effects. The study demonstrated that standard VNS and investigational µVNS therapy can be safely administered and are clinically compatible for patients undergoing fMRI and 3T MR imaging scans with no adverse events when protocols and guidelines are followed.8,9 Modest sample size, lack of a control group, unblinded status, and use of a single VNS model limits generalizations to other devices.
Additionally, any deviations from the equipment and protocols used in this study may pose additional risks. Further investigation with larger randomized, controlled trials is needed to confirm the findings of this study.
CONCLUSIONS
Standard VNS and investigational µVNS devices are safe during fMRI without device removal, provided certain restrictions are followed. Active VNS stimulation during MR imaging and fMRI is also safe without the risk of adverse events. The ability to perform fMRI during active standard and microburst stimulation is an important tool to understanding the mechanism of VNS and may be a valuable biomarker for stimulation optimization.
Acknowledgments
The authors acknowledge Amy Keith for her assistance with the project and Ryan Verner, PhD, for his assistance with the manuscript.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 9, 2024.
- Accepted after revision March 5, 2024.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.