
Abstract
BACKGROUND AND PURPOSE: Endovascular placement of coronary balloon-expandable stents in patients with recurrent cerebral ischemia has emerged as a treatment option for intracranial arterial occlusive disease. We have developed an in vitro model matching the tortuous curve of the carotid siphon that allows the assessment of apposition of stents to a curved vessel wall.
METHODS: Six types of balloon-expandable coronary stents were implanted in a silicone model of the carotid siphon. Digital radiographs and 3D rotational angiograms were obtained. Stent morphology was evaluated and the degree of apposition between stent and wall of the model was measured on a digital workstation.
RESULTS: All 6 stents showed lack of apposition between stent and the wall at the convexity of the anterior segment of the carotid siphon and the wall at the concavity at both extremities of the stent. In and around the curve, the modules of the stents did not expand completely to their nominal diameter and were distorted to an oval shape.
CONCLUSION: The tested coronary balloon-expandable stents did not completely conform to the vessel wall of the model of the carotid siphon and further development is needed to approach the goal of an “ideal intracranial stent.”
Endovascular stent placement in patients with recurrent cerebral ischemia has emerged as a treatment option for intracranial artery occlusive disease. Several case series have demonstrated the feasibility of stent placement and have shown a reduction of stenosis after stent implantation.1–3 The development of compact and more flexible balloon-expandable coronary stents has allowed access to intracranial lesions and encouraged the off-label use of such devices in patients with intracranial arterial stenosis.
In many respects, however, the intracranial vessels differ from the coronary vessels. Therefore, stents designed specifically for coronary use may not meet the exact requirements of intracranial vessels. The characteristics of the stent system will ultimately affect the safety of intracranial procedures as well as the long-term vessel patency.
The muscle layer of the tunica media of intracranial arteries is thinner and the vessels are surrounded by subarachnoid space. As a result, the arteries are more fragile and prone to rupture and dissection. The tortuosity of the carotid siphon can hinder the navigation with a balloon-mounted stent to the anterior and middle cerebral artery. In addition, stent apposition may be compromised in a curved segment with a small radius such as the carotid siphon. Stent malapposition may lead to immediate flow reduction, embolic complications, and restenosis.
Intracranial stent placement frequently demands stent deployment into curved vessel segments. Previous studies of wall apposition of coronary stents were designed to simulate coronary anatomy4,5 and did not match the requirements for intracranial stent placement. The proximal and distal extent of the carotid siphon, unlike coronary and intracranial arteries within the subarachnoid space, are largely constrained by bony and dural structures. This limits the ability of the siphon itself to “conform” to a rigid stent.
Our aim is to develop an in vitro model matching the dimensions of the carotid siphon with its curve that allows the assessment of apposition of stents to a curved vessel wall. Different types of commercially available coronary stents are compared with regard to these parameters.
Methods
The model of the carotid siphon was an elastic silicone tube (Elastrat, Geneva, Switzerland). Liquid silicone was painted on a wax copy with dimensions derived from 3D rotational angiographies from human carotid siphons. The anatomy of the model is simplified representing an “open” siphon because it duplicates only the curve in the caudocranial dimension and not the lateral to medial curve in a human carotid siphon. The inner diameter of the tube was 3.5 mm. The siphon was simulated by a 180° curve with a middle radius of 3.5 mm. The model was mounted in an acrylic box and filled with a fluid mixture of 30% contrast medium (Ultravist 240; Schering, Berlin, Germany) and 70% water adjusted to 37°C temperature. Six currently available coronary stent types were implanted (Table 1).
Coronary balloon-mounted stents tested in silicone model
The stents were implanted over a 0.14-inch wire (TransEnd; Boston Scientific/Target, Fremont, Calif) under fluoroscopic guidance in the digital subtraction angiography (Allura; Philips, Eindhoven, the Netherlands) through a 6F introducer sheath. All stents were positioned in the model at the midportion of the angular point of the curve, and the balloons were inflated at the pressure appropriate to the nominal stent diameter as provided by the manufacturer. Straightening of the curve was limited during inflation of the balloon by banding of the curve with a synthetic ring to an outer diameter of 12 mm. After 20 seconds, the balloon was deflated and the wire was removed carefully. To avoid distortion of the stent, the balloon was left in place.
The stent in the model was captured with radiographs (Allura, Philips) with the following parameters: matrix, 1024; BV, 17 cm; 50 kV; 300 milliseconds, small focus. In addition, a 3D rotational angiogram was acquired and reconstructed to visualize the morphology of the stent after deployment.
To quantify the lack apposition of the stents to the vessel wall an apposition ratio was defined and calculated: area between stent and vessel wall in relationship to the area within the stent lumen.6 The apposition ratio was calculated as (A + C)/B, with A being the area between stent and the wall at the convexity of the anterior segment of the siphon, B being the area within the stent, and C being the area between stent and wall at the concavity at both extremities of the stent (Fig 1).

Measurement of apposition of the stent to the carotid siphon shaded in gray.
A, Area between stent and the wall at the convexity of the anterior segment of the siphon.
B, Area within the stent.
C, Area between stent and wall at the concavity at both extremities of the stent.
All measurements were undertaken twice on the radiographs by using a digital workstation (Easy Vision, Philips) by 2 observers (R.d.M.d.R., B.Y.), and the average value was taken. The measurements were calibrated by using the internal diameter of the model (3.5 mm) as reference.
Results
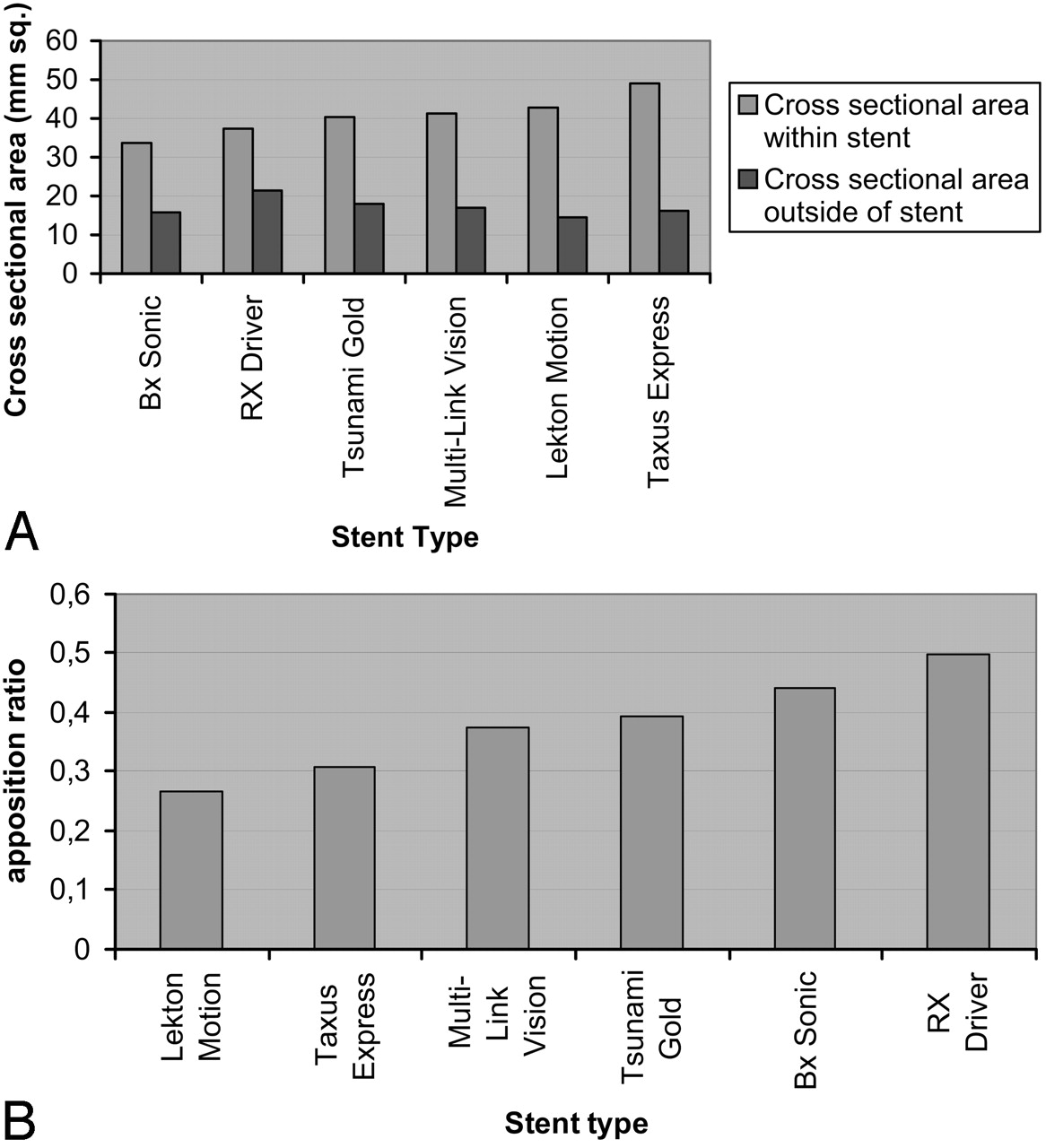
Digital radiographs and 3D images (volume-rendering technique) after implantation of 6 coronary stents into the model are shown in Fig 2. The measurements of the area between stent and vessel wall and of the area within the stent and the calculated apposition ratio are illustrated in Fig 3.

Digital images (1) and 3D rotational images (volume rendering) (2) of the 6 balloon-expandable stents after implantation in the silicone model of the carotid siphon (A) Cordis Bx Sonic, (B) Medtronic RX Driver, (C) Biotronik Lekton Motion, (D) Guidant Multi-Link Vision, (E) Boston Scientific TAXUS Express2, and (F) Terumo Tsunami Gold. Note the limited conformability especially to the outer curve.

A, Measurements of the area within the stent (first bar). The summation of the area between stent and the wall at the convexity of the anterior segment of the siphon and the wall at the concavity at both extremeties of the stent (second bar) for all tested stents.
B, Apposition ratio: area between stent and vessel wall in relationship to the area within the stent.
All 6 stents showed lack of apposition between the stent and the wall at the convexity of the anterior segment of the carotid siphon and the wall at the concavity at both extremities of the stent. The stents had not expanded completely to their nominal diameter in the midportion and were distorted to an oval shape. There was minor kinking at the concavity of the stent, but no complete collapse visible on 3D images. The calculated apposition ratio (Fig 3) showed that the Biotronik Lekton Motion had the best apposition to the curved vessel segment.
Discussion
Balloon-expandable coronary stents are used off-label for the treatment of intracranial arterial occlusive disease in patients with recurrent cerebral ischemia.
The tortuosity of the intracranial vascular system differs from the coronary vascular system, requiring special features of the stent systems. The characteristics of the stent system will affect the safety of the procedure as well as the long-term results. Incomplete stent apposition is associated with increased risk of restenosis in the coronary vascular system.7
In a simplified elastic silicone model of the human carotid siphon, we tested 6 currently available coronary stent systems. Visual evaluation and measurement of geometric parameters showed that the apposition of currently available balloon-expandable coronary stents is limited, especially the apposition of stent to the convexity of a curved vessel segment.
There are several limitations of the in vitro model experiment. First, the elastic properties of the silicone model are probably not similar to those in atheroma-ridden arteries with stenosis. Second, we tested only a single simplified geometric construction of the carotid siphon that duplicates the curve of the carotid siphon only in the caudal-cranial dimension and not the lateral to medial curve in a human carotid siphon. In addition, we tested only a single diameter (3.5 mm) of the model, which is at the lower extreme of normal intracavernous ICA diameter. Third, to avoid distortion of the stent during removal, the balloon was only deflated and left in place. The stiffness of the balloons might have contributed to poor apposition of the stents. The results, however, correspond with our clinical experience of limited wall apposition of stents in curved vessel segments.
Better conformability of stents may be achieved by reducing the number of connecting struts between the stent modules, but this can induce separation between the stent modules with plaque protrusion at the outer curve and modules overlaying each other at the inner curve. Another possible solution may be predilation of the arterial stenosis followed by deployment of a self-expanding stent (WingSpan, Boston Scientific),8 but the clinical experiences with this device are limited and the mechanical properties of the stent were not tested here.
Conclusions
The tested coronary balloon-expandable stents did not completely conform to the vessel wall of the model of the carotid siphon, and further development is needed to approach the goal of an “ideal intracranial stent.”
Footnotes
There are no potential conflicts of interest. Stents were provided by Biotronik, Boston Scientific, Cordis, Guidant, and Terumo.
References
- Received April 28, 2005.
- Accepted after revision June 14, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}