
Abstract
BACKGROUND AND PURPOSE: The pathophysiology underlying idiopathic intracranial hypertension (IIH) remains incompletely understood. While one theory postulates impaired cerebral glymphatic clearance in IIH, there is a paucity of methods to quantify glymphatic activity in human brains. The purpose of this study was to use advanced diffusion-weighed imaging to evaluate the glymphatic clearance of IIH patients and how it may relate to clinical severity.
MATERIALS AND METHODS: DWI was used to separately evaluate the diffusivity along the cerebral perivascular spaces and lateral association and projection fibers, with the degree of diffusivity used as a surrogate for glymphatic function (diffusion tensor image analysis along the perivascular space. Patients with IIH were compared with normal controls. Glymphatic clearance was correlated with several clinical metrics, including lumbar puncture opening pressure and Frisen papilledema grade (low grade: 0–2; high grade: 3–5).
RESULTS: In total, 99 patients with IIH were identified and compared with 6 healthy controls. Overall, patients with IIH had significantly lower glymphatic clearance based on DWI-derived diffusivity compared with controls (P = .005). Additionally, in patients with IIH, there was a significant association between declining glymphatic clearance and increasing Frisen papilledema grade (P = .046) but no correlation between opening pressure and glymphatic clearance (P = .27). Furthermore, healthy controls had significantly higher glymphatic clearance compared with patients with IIH and low-grade papilledema (P = .015) and high-grade papilledema (P = .002). Lastly, patients with IIH and high-grade papilledema had lower glymphatic clearance compared with patients with IIH and low-grade papilledema (P = .005).
CONCLUSIONS: Patients with IIH possess impaired glymphatic clearance, which is directly related to the extent of clinical severity. The DWI-derived parameters can be used for clinical diagnosis or to assess response to treatment.
ABBREVIATIONS:
- AQP
- aquaporin
- AUC
- area under the curve
- DTI-ALPS
- DTI analysis along the perivascular space
- FA
- fractional anisotropy
- IIH
- idiopathic intracranial hypertension
- ROC
- receiver operating characteristic
Idiopathic intracranial hypertension (IIH) is a disease characterized by increased intracranial pressure of unknown etiology.1 While generally considered multifactorial, a principal underlying process driving IIH pathophysiology has yet to be identified. A small number of groups have recently theorized that IIH might primarily be a consequence of abnormally functioning cerebral glymphatics with impaired clearance of CSF and cerebral interstitial fluid.2⇓-4 Broadly, the cerebral glymphatic system is a “brain-wide pathway for fluid transport, which includes the para-arterial influx of subarachnoid CSF into the brain interstitium, followed by clearance of interstitial fluid along large-caliber draining veins.”5 Nonetheless, experimental evidence supporting the dysfunctional glymphatic model for IIH remains sparse, largely due to a paucity of methods to measure glymphatic flow within the human brain.
Recently, MR imaging has been leveraged to noninvasively evaluate the cerebral glymphatic system.6⇓⇓⇓-10 More specifically, the diffusion tensor image analysis along the perivascular space (DTI-ALPS) technique has emerged as a robust imaging method to quantify the degree of glymphatic clearance and has been used in numerous prior studies.6⇓⇓⇓-10 DTI-ALPS allows the assessment of glymphatic activity without intravenous or intrathecal contrast agent injection. The glymphatic clearance assessed with DTI-ALPS has been shown to be correlated with that assessed with the direct intrathecal tracer-based measurement in humans.6⇓⇓⇓-10 In short, the DTI-ALPS method measures the diffusivity along the perivascular space compared with projection and association fibers adjacent to the lateral ventricle body, and serves as a measure of glymphatic outflow.5⇓⇓⇓⇓-10 Here, we hypothesized that patients with IIH possessed impaired glymphatic clearance that could be directly identified and measured by using the DTI-ALPS method.
MATERIALS AND METHODS
Patient Cohort
In this retrospective study, approved by our Institutional Research Subject Review Board (STUDY00008280), 99 patients with clinically diagnosed IIH were retrospectively identified from our single-center tertiary care institution from 2016 to 2023. A small set of healthy controls (n = 6) were also retrospectively identified who possessed no significant medical history (including no history of chronic headaches), and had normal brain MRIs. All subjects had previously undergone MR imaging as part of their standard of care (performed as part of a standardized MR imaging protocol), including structural T1-weighted imaging and DWI with 12 or 14 directions.
Inclusion and Exclusion Criteria
Patients with clinically diagnosed IIH were enrolled according to diagnostic criteria as previously described by Friedman et al.11 Patients with no other confounding neurologic disorders (eg, brain tumor, migraine, multiple sclerosis, meningitis, etc) were retrospectively identified based on the inclusion of a T1-weighted scan and DWI with at least 12 directions. All imaging was completed within 3 months of clinical diagnosis and before any medical or interventional treatment. Patients up to the age of 50 were eligible for inclusion; patients older than 50 years were excluded because increasing age and small vessel disease have been shown to influence ALPS index and may function as a confounding variable.6,12
Clinical Data
Clinical data on IIH patient demographics, presenting clinical features, and pertinent past medical history were collected and presented. Furthermore, documented Frisen papilledema grade at time of initial presentation and diagnosis was collected along with lumbar puncture opening pressure in the lateral decubitus position.
Image Acquisition
All images were acquired on a 3T Discovery 750 MR imaging system (GE Healthcare) with an 8-channel head coil. Anatomic T1-weighted imaging was acquired as well as a standard clinical DTI protocol with 12–14 diffusion-weighted directions with b = 1000 seconds/mm2 and 4 b = 0 reference images.
Quantification with DTI-ALPS
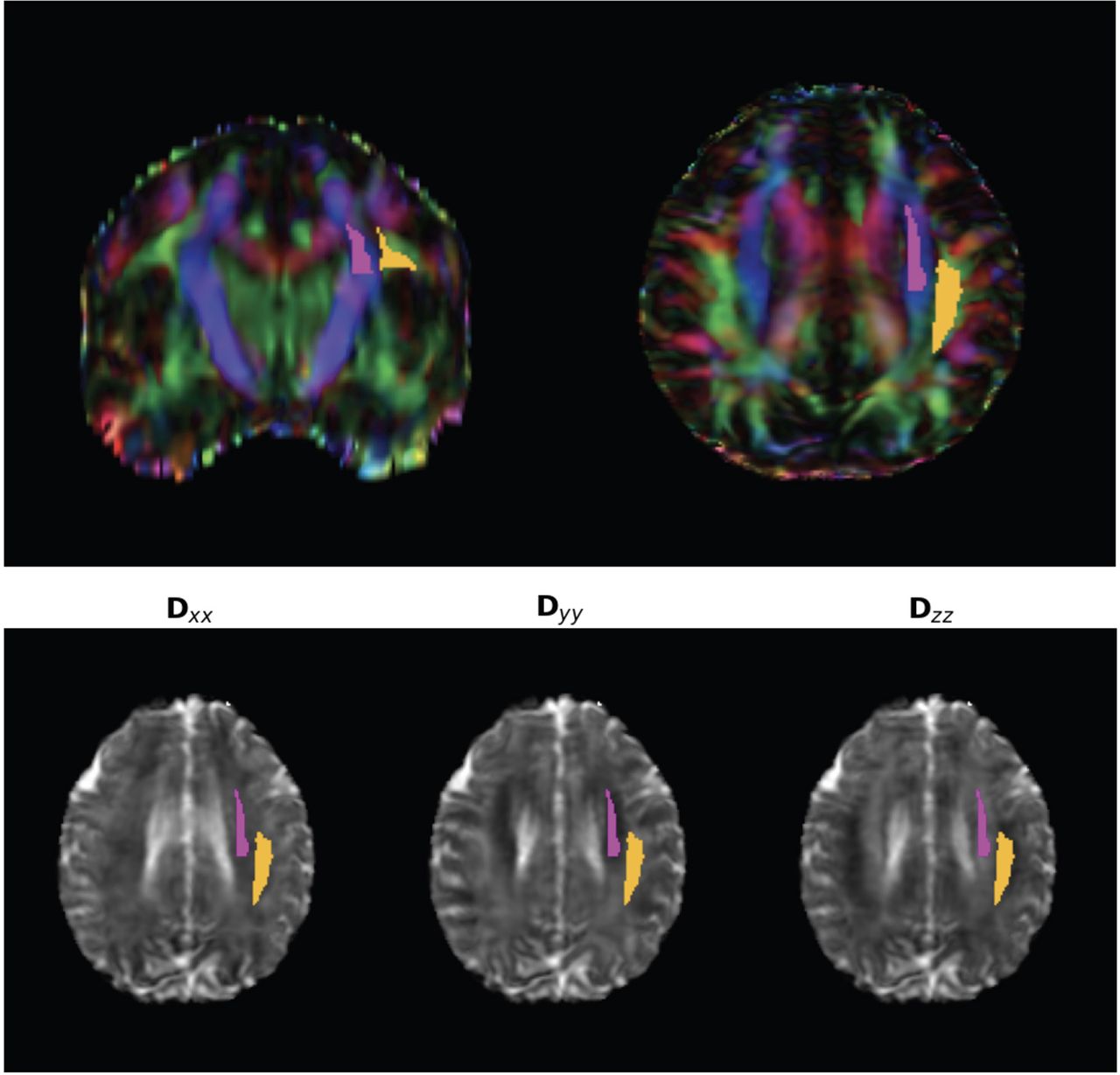
This study leveraged the DTI-ALPS technique to quantify the degree of cerebral glymphatic function, which has been well described in prior studies.6⇓⇓⇓-10 DWI data were corrected for eddy current-induced distortion by using EDDY_CORRECT in FSL (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/eddy). Susceptibility-induced distortion was corrected by using INVERSION consisting of inverse contrast normalization of T1-weighted data and diffeomorphic coregistration by using symmetric normalization in ANTs (http://stnava.github.io/ANTs/).13 Diffusivity maps along the x-axis (Dxx), y-axis (Dyy), and z-axis (Dzz) were computed in addition to fractional anisotropy (FA), mean diffusivity, axial diffusivity, and radial diffusivity by using DIPY (https://dipy.org/index.html). FA maps were coregistered to the FA map template FMRIB58 atlas by using ANTs. The FA registration matrix was used to warp all other DTI maps to standard space. Modified JHU ICBM white matter labels were used for the projection (superior corona radiata) and association fibers (superior longitudinal fasciculus) in the periventricular area.14 As a quality assurance step, ROIs were defined in standard (MNI) space, and all diffusion directions were warped to MNI space. In addition, all subjects were individually reviewed for correct registration and ROI placement. An example atlas-based ROI determination can be seen in Figure 1. In accordance with prior studies, the DTI-ALPS index, which is used as a measure of glymphatic flow, was then computed by using these labels, defined by the following:


ROI by using atlas-based ALPS index. Top row: The projection (superior and posterior corona radiata, magenta) and association (superior longitudinal fasciculus, yellow) fibers were defined by the labels of the ICBM DTI-81 Atlas. Bottom row: Gray-scale maps of X, Y, and Z diffusion with ROIs.
Statistical Analysis
Correlations among continuous variables (opening pressure, Frisen papilledema grade, ALPS index, etc) were performed via linear regression. Differences between and among groups were assessed by an unpaired, 2-tailed t test or 1-way ANOVA. Additionally, receiver operating characteristic (ROC) curve analysis with calculation of the area under the curve (AUC) was completed to assess the diagnostic performance of the ALPS index for patients with IIH versus controls and between less-severe and more-severe IIH cases. All statistical analyses were completed and graphed by using GraphPad Prism statistical software (version 10). For all statistical tests, a P value of ≤.05 was used to indicate statistical significance.
RESULTS
Patient Clinical Characteristics
A total of 99 patients with clinically diagnosed IIH with sufficient MR imaging sequences for analysis were retrospectively identified. The average age at diagnosis was 29 years (SD: 8 years), 88% were female, and the average body mass index was 40.7 (SD: 8.3). Regarding presenting clinical features, 90% presented with a headache, 69.7% had visual disturbance, 94% had papilledema at presentation, and the mean opening pressure on lateral decubitus lumbar puncture was 37.6 cmH20 (SD: 9.4). Frisen papilledema grade was explicitly documented in 81 of the patients with IIH (median grade = 2). MRV was completed in 91 (92%) patients with IIH, and some degree of venous sinus stenosis was present in 82 (90%) cases. Complete pertinent clinical characteristics of the patients with IIH are shown in the Online Supplemental Data. Regarding healthy controls, 6 female patients were identified with a mean age of 25.2 (SD: 2.3) and mean body mass index of 27.2 (SD: 6.3). There was no significant difference in mean age between patients with IIH and controls (P = .2). These 6 controls had normal brain MRIs and had no significant past medical history, including no history of chronic headaches.
Glymphatic Clearance and DWI Analysis
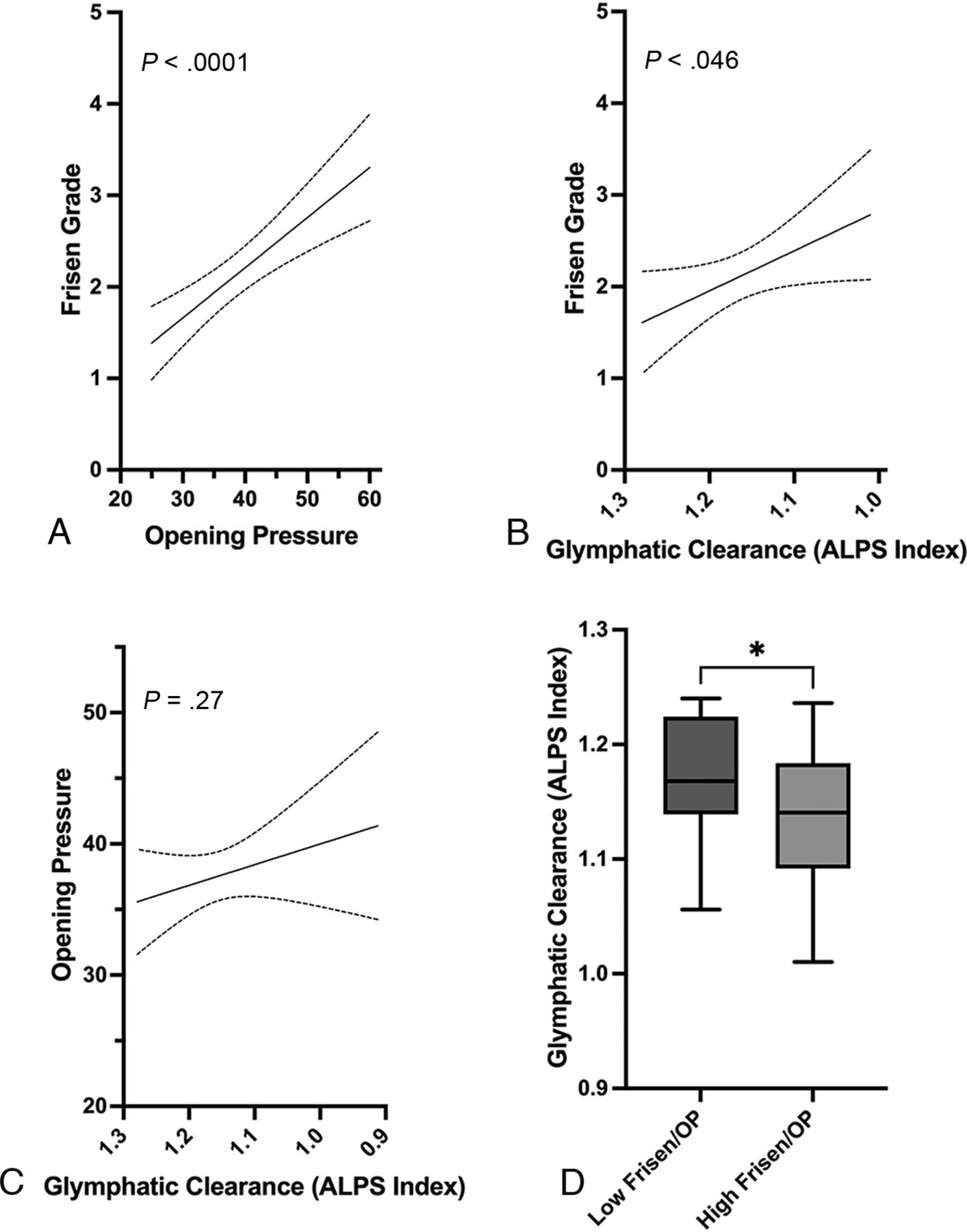
First, there was no statistical difference in the number of DTI diffusion directions between the subjects (mean, 17.529; SD: 9.4) and controls (mean, 16.5; SD: 4.5) (P = .45). Overall, control patients had significantly higher glymphatic clearance (ALPS index mean, 1.23; SD, 0.04; coefficient of variation: 3.2%) compared with patients with IIH (mean, 1.15; SD, 0.07) (P = .005). Additionally, there was a significant correlation between worsening/increasing Frisen papilledema grade and lumbar puncture opening pressure within the patients with IIH (P < .0001) (Fig 2A). There was also a significant association between declining glymphatic clearance and worsening Frisen grade (P = .046) (Fig 2B). However, there was no significant relation between glymphatic outflow and lumbar puncture opening pressure (P = .27) (Fig 2C). Given the significant association between Frisen grade and opening pressure (Fig 2A), we hypothesized that there may be a difference in glymphatic clearance between patients with IIH and both low Frisen grade (0–2) and lower opening pressure (<50 percentile of cohort) compared with patients with both high Frisen grade (≥3) and higher opening pressure (≥50 percentile). We found that patients with both a high Frisen grade and higher opening pressure had significantly lower glymphatic clearance compared with those with a low Frisen grade and lower opening pressure (P = .029) (Fig 2D).

A, Association between lumbar puncture opening pressure and Frisen papilledema grade in patients with IIH. B, Association between glymphatic function (ALPS index) and Frisen papilledema grade. The glymphatic clearance on the x-axis is declining moving left to right. C, Association between glymphatic clearance and lumbar puncture opening pressure in patients with IIH. D, Box-and-whisker plot showing difference in glymphatic clearance between patients with IIH and low Frisen grade papilledema (0–2) and lower opening pressure (<50th percentile in cohort) compared with patients with IIH and high Frisen grade papilledema (3–5) and higher opening pressure (≥50th percentile). * indicates P < .05.
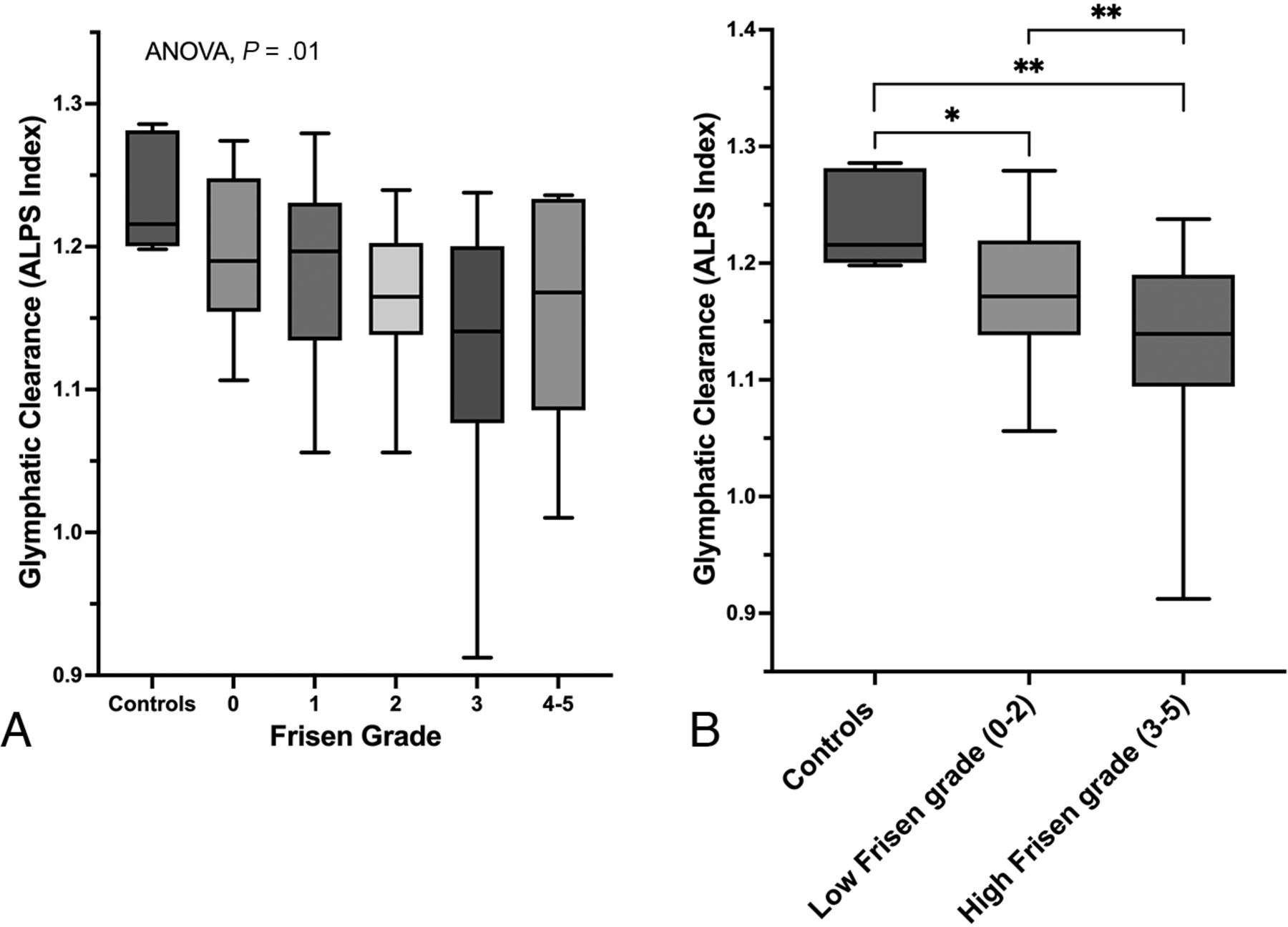
Because we found that glymphatic clearance was significantly associated with the clinical severity of papilledema (Fig 2B), we investigated how the glymphatic outflow of controls compared with patients with IIH and varying Frisen grade. Between-groups ANOVA test demonstrated significantly different degrees of glymphatic clearance between controls and different Frisen grades (P = .01, Fig 3A). Furthermore, patients with low Frisen grade (0–2) papilledema had significantly lower glymphatic clearance compared with controls (P = .015). Similarly, patients with high Frisen grade papilledema (3–5) also had significantly lower glymphatic clearance compared with healthy controls (P = .002). Last, patients with IIH and high-grade papilledema also had significantly lower glymphatic clearance compared with patients with IIH and low-grade papilledema (P = .005) (Fig 3B).

A, Box-and-whisker plot showing glymphatic clearance and how it relates between controls and patients with IIH and varying Frisen papilledema grades. B, Box-and-whisker plot showing difference in glymphatic clearance between controls and patients with IIH and low-grade papilledema (Frisen grade 0–2) and high-grade papilledema (Frisen grade 3–5). * indicates P < .05; ** indicates P < .01.
ROC Curve Analysis
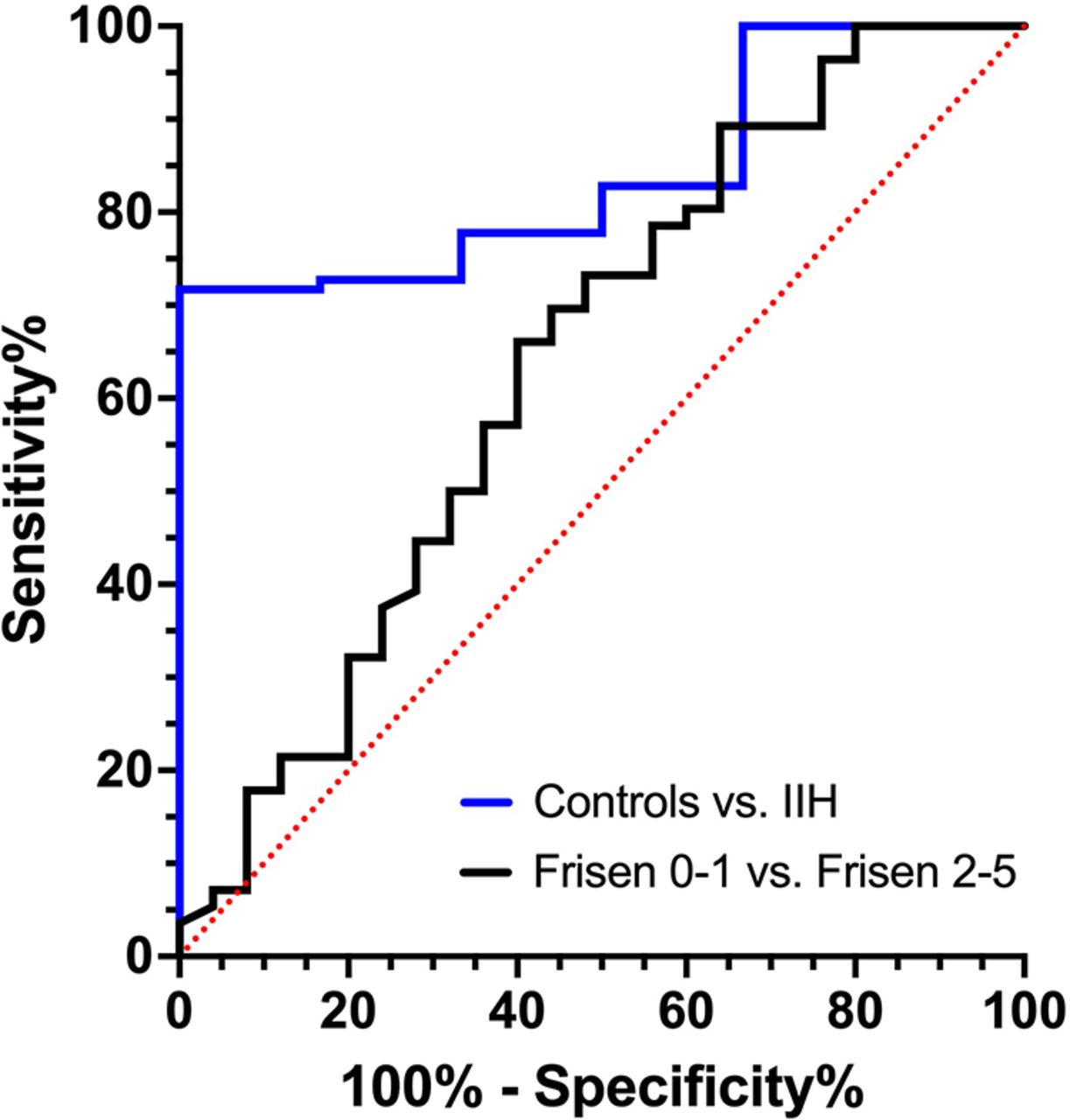
ROC curve analysis was completed to assess the diagnostic performance of the ALPS index between IIH cases versus controls and between patients with IIH and less-severe (Frisen grade 0–1) and more-severe (Frisen grade 2–5) cases. Regarding IIH cases versus controls, ROC curve analysis demonstrated an AUC of 0.842 (SD, 0.06, P = .005), where an ALPS index of <1.197 was found to have a sensitivity of 71.7% and a specificity of 100% (Fig 4). When comparing less-severe IIH cases to more-severe IIH cases, ROC curve analysis demonstrated an AUC of 0.64 (SD: 0.07, P = .045), where an ALPS index of <1.179 had a sensitivity of 66.1% and a specificity of 60% (Fig 4). However, when comparing Frisen grade 0–2 versus Frisen grade 3–5, ROC curve analysis was not statistically significant (AUC: 0.62, P = .06).

ROC curve analysis assessing the diagnostic performance of the ALPS index between patients with IIH versus controls and between patients with IIH and less-severe (Frisen papilledema grade 0–1) and more-severe (Frisen papilledema grade 2–5) disease.
DISCUSSION
This study used the DTI-ALPS technique to evaluate the cerebral glymphatic system in patients with IIH. We found that overall patients with IIH had significantly lower glymphatic clearance compared with healthy controls (P = .005). Additionally, we found a direct association between worsening clinical papilledema and declining glymphatic clearance (P = .046). Moreover, this study demonstrated that, compared with controls, patients with IIH had lower glymphatic clearance with both low-grade (P = .015) and high-grade papilledema (P = .002). Overall, these findings suggest that there is impaired glymphatic clearance in IIH and that the degree of impaired clearance is directly associated with degree of clinical severity.
The pathophysiology of IIH remains incompletely understood. Though many consider the pathophysiology to be multifactorial, there is a developing hypothesis that IIH is principally due to impairment of the cerebral glymphatic system.2,3 Likewise, some have postulated a link between aquaporin-4 (AQP4) alterations and impaired glymphatic outflow resulting in IIH.2,15 However, this hypothesis is largely theoretical with limited experimental evidence to substantiate that glymphatic dysfunction is actually present in IIH. One of the reasons for this is a paucity of methods to evaluate the glymphatic system in patients.
While data are overall sparse, a few studies have suggested that impaired glymphatic flow is present in IIH. One of the first studies to suggest glymphatic dysfunction in IIH was by Alperin et al16 who compared 11 patients with IIH with 11 controls by using MR imaging and showed increased gray matter interstitial volume in patients with IIH. Additionally, a prior study by using gadobutrol MR imaging tracer compared 15 patients with IIH with 15 controls and found delayed tracer clearance in patients with IIH, suggesting impaired glymphatic clearance.17 It has also been shown that patients with IIH possess a higher quantity of cerebral perivascular spaces, a suspected pathway of the glymphatic system, which has indirectly suggested impaired glymphatic outflow in IIH.18
The presented analysis is the first study to demonstrate that the magnitude of glymphatic clearance as defined with diffusion measurement in IIH is directly associated with the extent of clinical severity (Figs 2B, 3B), suggesting that impaired glymphatic clearance underlies IIH pathophysiology and may drive disease. These findings, combined with impaired cerebral venous outflow thought to be involved in IIH, further suggest that IIH is a “glymphedema” of the brain.19 Likewise, it has been previously hypothesized by Alperin et al16,20 that resistance to cerebral venous return is the potential genesis leading to increased brain interstitial volume. Together, this could suggest that impaired cerebral venous return — possibly, via venous sinus stenosis, or other mechanisms — results in veno-glymphatic congestion and either causes or exacerbates the observed impaired glymphatic clearance. Future studies may investigate how diffusivity is related to extent of venous collaterals or degree of venous sinus stenosis.
Nonetheless, while our findings provide evidence for the IIH glymphatic dysfunction model, the underlying molecular mechanisms have yet to be elucidated. However, it has been theorized that defective AQPs involved in cerebral fluid transport and glymphatic outflow may be dysfunctional in IIH, possibly due to hormonal or genetic alterations.2 Likewise, AQP4 has been shown to regulate water transport between the brain and CSF,5 and has also been shown to be differentially expressed in IIH.21 Similarly, AQP1 has been implicated in drug-induced IIH.22 Regardless, further research is required to unravel the molecular mechanism between IIH and possible glymphatic dysfunction. Also, additional imaging analysis of other DTI parameters, such as perfusion or chemical exchange saturation transfer imaging, may yield clinically meaningful insights in patients with IIH.
This study has several limitations that need to be considered. First, this is a single-center retrospective analysis, which subjects it to the inherent biases of this study design, such as selection bias of the included participants. In addition, recent work has shown the ALPS index to be a robust metric across scanning parameters, but that it can vary with the number of diffusion-weighting directions.6 Additionally, an obvious limitation is the small number of healthy controls within our cohort (n = 6). Given the retrospective design of this study, identifying healthy controls without any significant possibly confounding medical history, and with adequate MR imaging sequences for analysis, is challenging. Nonetheless, even with such a small number of controls, we still detected a significant overall difference in glymphatic clearance in patients with IIH (Fig 2). Moreover, we found that papilledema grade was directly related to the extent of impaired glymphatic clearance in IIH, which is inherently a control-independent analysis (Figs 2B, 3B). Regardless, we believe that future studies investigating the glymphatic system in patients with IIH should ideally be prospectively designed and with a larger number of controls.
CONCLUSIONS
Based on DWI-derived diffusivity, patients with IIH possess impaired glymphatic clearance that correlates with the extent of disease severity, providing further evidence that primary glymphatic dysfunction may underlie IIH pathophysiology. These DWI-derived parameters can also be used for clinical diagnosis or to assess early response to treatment. Further studies are needed to assess the efficacy of DTI-ALPS as a diagnostic and prognostic biomarker in patients with IIH.
Footnotes
Supported by the Department of Imaging Sciences, University of Rochester Medical Center, Fischer Fund Grant. Supported in part by National Institutes of Health Grants R01MH118020 and R01AG054328.
Derrek Schartz and Alan Finkelstein contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
REFERENCES
- Received August 14, 2023.
- Accepted after revision November 2, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Total brain volume is associated with severity of transverse sinus stenosis in idiopathic intracranial hypertension
- Glymphatic Flow after Thrombectomy is Associated with Futile Recanalization in Large Vessel Occlusion Stroke
- Improved Cerebral Glymphatic Flow after Transvenous Embolization of CSF-Venous Fistula