
Abstract
BACKGROUND AND PURPOSE: Our aim was to assess the relationship between volume and percentage of intraplaque hemorrhage measured using CT and the occurrence of cerebrovascular events at the time of CT.
MATERIALS AND METHODS: One-hundred-twenty-three consecutive subjects (246 carotid arteries) with a mean age of 69 years who underwent CTA were included in this retrospective study. Plaque volume of components and subcomponents (including intraplaque hemorrhage volume) was quantified with dedicated software.
RESULTS: Forty-six arteries were excluded because no plaque was identified. In the remaining 200 carotid arteries, a statistically significant difference was found between presentation with cerebrovascular events and lipid volume (P = .002), intraplaque hemorrhage volume (P = .002), percentage of lipid (P = .002), percentage of calcium (P = .001), percentage of intraplaque hemorrhage (P = .001), percentage of lipid-intraplaque hemorrhage (P = .001), and intraplaque hemorrhage/lipid ratio (P = .001). The highest receiver operating characteristic area under the curve was obtained with the intraplaque hemorrhage volume with a value of 0.793 (P = .001), percentage of intraplaque hemorrhage with an area under the curve of 0.812 (P = .001), and the intraplaque hemorrhage/lipid ratio with an area under the curve value of 0.811 (P = .001).
CONCLUSIONS: Results of our study suggest that Hounsfield unit values <25 have a statistically significant association with the presence of cerebrovascular events and that the ratio intraplaque hemorrhage/lipid volume represents a strong parameter for the association of cerebrovascular events.
ABBREVIATIONS:
- AUC
- area under the curve
- IPH
- intraplaque hemorrhage
- ROC
- receiver operating characteristic
Several studies have demonstrated, in recent years, that the degree of stenosis should not be considered the only parameter to identify carotid plaque at risk of distal embolization and that additional plaque features can increase or reduce risk of plaque rupture and embolic events.1⇓⇓–4 In particular, intraplaque hemorrhage (IPH) has been convincingly associated with a higher risk of ipsilateral cerebrovascular events.5,6
Although MR imaging has been widely used to identify IPH,7⇓–9 recent evidence suggests that CT,10 using a threshold of attenuation values of <25 HU in the carotid artery, can consistently identify the presence of IPH. Moreover, with improved algorithmic and hardware evolution, there has been an increasing role of volumetric quantification of tissue components for plaque characterization.11⇓⇓–14
In the present study, we assessed the relationship between volume and the percentage of IPH measured using software analysis in volumetric CT and the occurrence of cerebrovascular events (stroke and TIA).
Materials and Methods
Study Design and Patient Population
Institutional review board approval for this study was obtained, and patient consent was waived because of the retrospective nature. On the basis of a power calculation (type I error, α = .05; type II error, β = 0.1; area under the curve [AUC] null hypothesis value = 0.5; AUC significant value = 0.7, pooled group), we estimated that a sample size of at least 130 (with a 30% IPH prevalence) carotid arteries would be sufficient to investigate the potential effect of CT-detected IPH versus the occurrence of cerebrovascular events. We decided to also include a correction factor of 10%, yielding a necessary sample size of 143 carotid arteries. Moreover, because in each subject, there are 2 carotid arteries and this determined a bias in the model, we decided to study 200 carotid arteries to avoid the inference determined by the 2 carotid arteries in each patient.
Consecutive subjects who underwent CT of the carotid arteries in our hospital from March 2013 were included until the threshold of 200 carotid arteries was reached (January 2014) for a total of 246 carotid arteries in 123 subjects (94 men, 29 women; mean age, 69 years; age range, 45–86 years). For each subject, when both carotid arteries showed atherosclerotic plaque, the left and right sides were included. Plaque was defined according to the Mannheim consensus15 as a carotid wall thickness of >1500 μm.
In cases in which only 1 carotid artery was pathologic, the normal side (46 carotid arteries) was excluded from analysis, leaving 200 arteries with an atherosclerotic plaque for analysis.
Quantification of the degree of stenosis and plaque analysis was performed using CTA according to previously published criteria.16,17 Carotid sonography is used as a screening tool to identify carotid stenosis, and CTA was performed under the following circumstances: 1) Carotid sonography showed a pathologic stenosis (>50% measured with the NASCET criteria18) or features related to plaque vulnerability (ulcerations, irregular surface); 2) sonography could not adequately assess the degree of stenosis and plaque characteristics because of anatomic conditions; 3) diabetes screening; and 4) presurgery analysis. Moreover, all subjects with cerebrovascular events underwent CTA of the carotid arteries. The neurologic status at the time of CT was classified as symptomatic or asymptomatic according to the neurologic assessment documented in the clinical chart review using the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.19,20 The maximum timing between events and imaging to consider a subject as symptomatic was 1 week. In the case of >1 week between ischemic symptoms and CTA of carotid arteries, the patient was excluded. We defined as symptomatic those patients with TIA or stroke, considering TIA as a brief (<24-hour) episode of neurologic dysfunction such as dysarthria, dysphasia, hemiparesis, or hemiparesthesia and monocular blindness. If the episodes of neurologic dysfunction lasted >24 hours, the patient was considered to have a stroke. In case of doubt with other pathologies (eg, hypoglycemia, migraine, postparoxysmal neurologic dysfunction), we excluded patients from the analysis. Asymptomatic patients had no history of either remote or recent symptoms at the time of the examination. Clinical classification into symptomatic and asymptomatic was based on the assessment of the clinician evaluating the patient and ordering the diagnostic study and was extracted from the chart. We considered symptomatic patients those who had plaque in the carotid artery ipsilateral to the cerebrovascular event.
Moreover, we excluded patients with the following conditions: 1) concomitant intracranial pathology such as brain tumor, abscess, and encephalitis; and 2) the presence of a cardioembolic source documented by a cardiologist.
CTA Technique
Patients were studied using a 16–detector row CT system (Brilliance; Philips Healthcare, Best, the Netherlands). CT images were obtained with coverage from the aortic arch to the carotid siphon in a caudocranial direction, and examinations were performed before and after the administration of contrast material. An angiographic phase was obtained with the administration of 80 mL of prewarmed contrast medium, Ultravist 370 (iopromide; Bayer HealthCare, Berlin, Germany) into a cubital vein using a power injector at a flow rate of 4–5 mL/s and a 16-ga intravenous catheter followed by 30 mL of saline flush. CT technical parameters included the following: section thickness = 0.6 mm, section interval = 0.3 mm, matrix size = 512 × 512 pixels, FOV = 14–19 cm. A C-filter algorithm of reconstruction was applied.
IPH and Plaque Volume Component Analysis Quantification
Two radiologists (L.S. and A.B. with 11 and 8 years of experience in CTA, respectively) blinded to clinical information regarding symptomatic status performed all measurements of Hounsfield units using as window/level settings, W = 850:L = 300.21 Volume analysis was performed with dedicated software (Elucid Bioimaging, Wenham, Massachusetts) to semi-automatically quantify the subcomponent volume.22,23 With this software, it is possible to identify attenuation values of all the voxels within a volume, and by means of applying some thresholds, it is possible to classify the tissues according to the attenuation values (Fig 1). For this analysis, we considered 5 classes: 3, as suggested by de Weert et al24 in which voxels identifying lipid tissues were <60 HU, fibrous tissue between 60 and 130 HU, and calcium tissue >130 HU.10,24 Two additional classes (4 and 5) were added by splitting the lipid: the fourth class was the IPH for values <25 HU according to the findings by Saba et al,10 whereas the fifth class was the lipid-IPH, which included all the voxels with Hounsfield unit values between 26 and 59 HU.

The first case is a 69-year-old male patient with right stroke who underwent CTA that showed a large IPH component of 107 mm3 (A–C). A, The coronal view of the carotid CTA is given with the segmentation of the software (white open arrow). B, A coronal cut of the postprocessed carotid arteries is shown (white arrowhead). C, The white arrow indicates the internal carotid artery in the axial selected section. The legend of the chromatic scale is the following: red = IPH; yellow = lipid-IPH component; blue = mixed component; green = calcified component. The second case is a 73-year-old male patient with left MCA stroke with an IPH/lipid ratio of 0.93 (D–F). D–F, Three axial slices from the bifurcation upward were selected showing the presence of a large IPH and the small amount of lipid-IPH (white arrowheads).
We also calculated the percentages of these components, and finally, a ratio was introduced as the ratio of IPH/lipid volume (with values between 0, if no IPH was present, and 1, if all the lipid plaque component was due to IPH).
IPH Volume Dichotomization
After the volume calculation of the IPH, 5 thresholds were selected to obtain a dichotomization and subsequently test the effect of the presence/absence of IPH versus symptoms using a 6-hypothesis scenario. We considered the following 6 thresholds of IPH volume: 10, 50, 100, 150, 200, and 250 mm3.
Statistical Analysis
In this study, continuous data were described as the mean ± SD. Receiver operating characteristic (ROC) curve analysis was performed between volume and volume subcomponents (lipid, mixed, calcified, IPH, lipid-IPH tissue), percentage of variable of the subcomponents, ratio of IPH/lipid, and the presence of cerebrovascular events. The normality of each continuous group was tested using the Kolmogorov-Smirnov Z-test, and different values in groups with and without cerebrovascular symptoms were compared using the Mann-Whitney test. The dichotomized IPH values according to the thresholds were tested versus the presence/absence of cerebrovascular events using a χ2 test. A P value < .05 indicated a statistically significance association, and all values were calculated using a 2-tailed significance level. Statistical analysis was performed with the SPSS 13.0 Statistical Package (IBM, Armonk, New York). Graphics were plotted with MedCalc 15.0 software (MedCalc Software, Mariakerke, Belgium).
Results
General Results
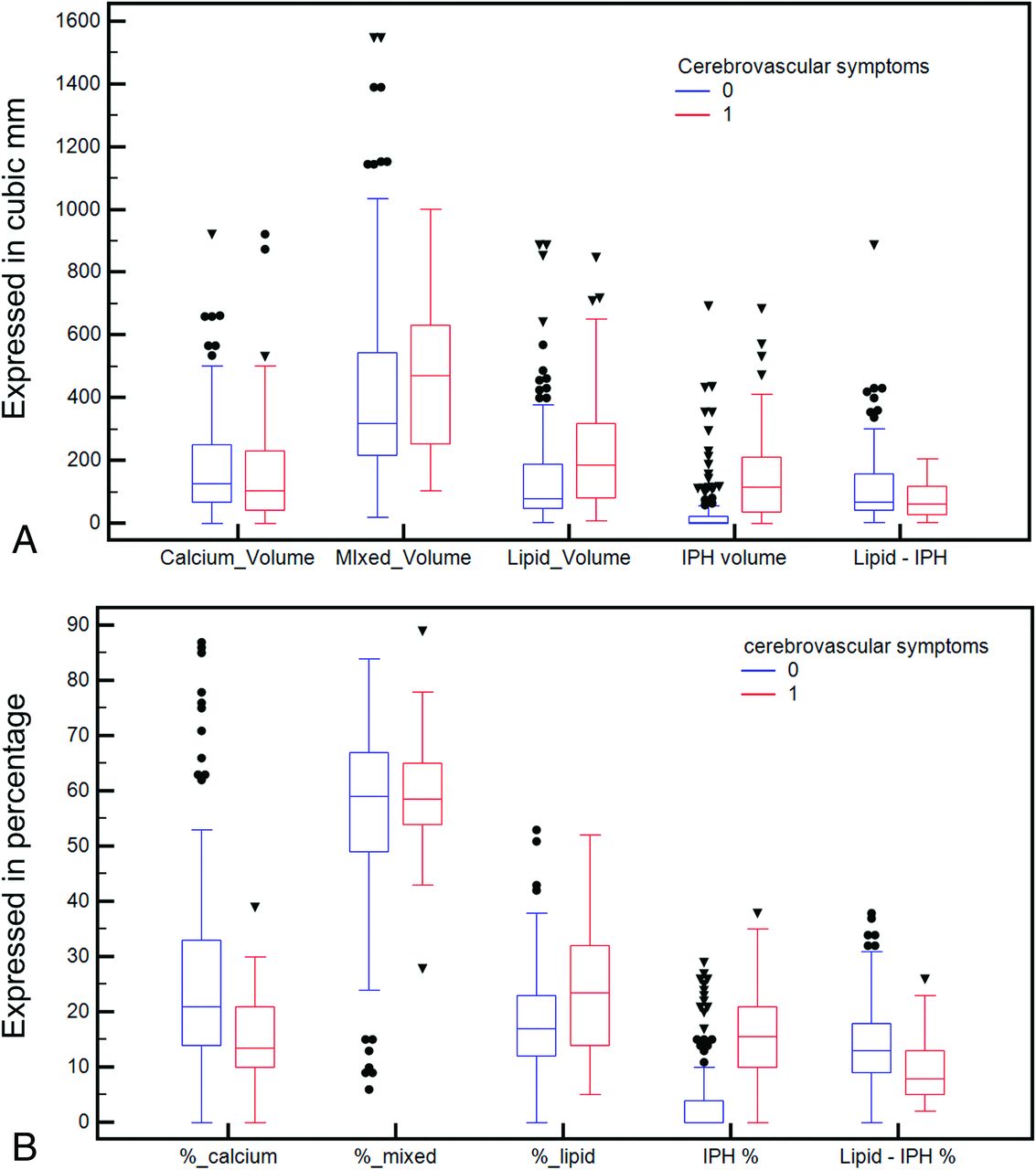
No patients were excluded due to suboptimal image quality. Of the 123 patients, 46 were symptomatic (15 strokes, 31 transient ischemic attacks) and 77 were asymptomatic. General plaque characteristics and their subcomponent volume and percentages are summarized in Table 1. No statistically significant difference was found for the common cerebrovascular risk factors between symptomatic and asymptomatic patients. However, there were statistically significant differences in the lipid volume (P = .002), IPH volume (P = .001), percentage of lipid (P = .002), percentage calcium (P = .001), percentage of IPH (P = .0001), percentage of lipid-IPH (P = .0001), and the IPH/lipid ratio (P = .001). Boxplots are given in Fig 2.

Boxplot of the volume components of the carotid artery plaque according to the presence or absence of cerebral symptoms (A) and boxplot of the percentages of the components according to the presence or absence of cerebrovascular symptoms (B).
Demographic and plaque characteristic summary table
ROC Curve Analysis
The ROC curve analysis for the total plaque component and subcomponent volume versus the presence of cerebrovascular symptoms is given in Fig 3A. Table 2 summarizes general ROC results from the volume analysis. The best ROC AUC was obtained with the IPH volume, with a value of 0.793 (P = .001).

ROC curve analysis of the volume components of the carotid artery plaque according to the presence or absence of cerebral symptoms (A) and ROC curve analysis of the percentages of the components according to the presence or absence of cerebral symptoms (B).
ROC curve analysis between symptoms and volume/percentage of plaque tissues
The ROC curve analysis was also performed for the percentage of plaque components versus the presence of cerebrovascular symptoms, and the ROC plot is shown in Fig 3B. Table 2 also summarizes the general ROC results from volume analysis. The best performance was obtained by the percentage of IPH with an AUC of 0.812; P = .001). Also, the IPH/lipid ratio showed a very good AUC, with a value of 0.811 (P = .001).
IPH Volume Dichotomization
In Table 3, the χ2 results for the different threshold volumes of IPH and cerebrovascular symptoms are summarized. The best association was found by considering a threshold of 50 mm3 (P = .001, χ2 = 43.913, contingency coefficient = 0.424).
χ2 test between symptoms and different volume thresholds of IPH
Discussion
Several studies have recently shown that carotid artery plaque characteristics are associated with a risk of rupture and subsequent distal embolization.2,3,5,24 In this study, we assessed the relationship between volume and percentage of IPH and other plaque components in the carotid artery detected with CT and their association with symptomatic status. We observed a significant association between the presence of ipsilateral cerebrovascular events and the absolute volume of IPH as well as plaque lipid content. Moreover, the ratio of IPH/lipid volume was strongly associated with cerebrovascular events.
Among factors involved with plaque rupture, IPH is one of the most dangerous, and its noninvasive identification is an important step for correct risk stratification.5⇓⇓–8 MR imaging is considered the best technique for the detection of IPH, while the value of CT is debated. However, a recent study10 suggests that a threshold of ≤25 HU is strongly associated with the presence of IPH on CT.
One of the main limitations of carotid plaque analysis was the fact that various imaging techniques do not account for the heterogeneous composition of the atherosclerotic tissue where several components can coexist in the same plaque.25,26 In the carotid artery plaque, coexistence of several components is frequent with changes across time. Volumetric analysis of the plaque could offer important insights because it allows us to quantify different plaque components and provides a more complete analysis.13,14,27,28 The introduction of a new CT criterion (≤25 HU of attenuation) for the detection of IPH applied to the use of volumetric quantification analysis systems could allow one to extrapolate the real impact of the IPH component. Recently published articles in 201929,30 have demonstrated that the volumetric analysis of the carotid artery plaques obtained by CT data is a reliable technique and that small changes in plaque composition can also be detected.30
In past years, the classic division of the carotid artery plaque type according to the attenuation values was based on the seminal study by de Weert et al,24 in which 3 classes were identified: lipid (<60 HU), mixed (between 60 and 130 HU), and calcified (>130 HU). With the demonstration that attenuation values of <25 HU are due to IPH,10 we tried to test the effect of the volumes for this component; therefore, the lipid class was divided into IPH (<25 HU) and lipid-IPH (from 26 to 59 HU). By comparing symptomatic with asymptomatic subjects, we found a statistically significant difference in volume for the lipid (P = .002), and in particular for the IPH volume (P = .001). These findings confirm that IPH volume is higher in plaques causing cerebrovascular events.2,3,5,6,31,32 Of interest, there was no difference in lipid-IPH volume tissue, whereas the total lipid volume showed a statistically significant difference. This finding can be explained because in the old classification the lipid volume class included all the voxels <60 HU (and therefore also the IPH component); these results suggest that tissues with an attenuation between 26 to 59 HU, namely fatty components, are not associated with the presence of cerebrovascular events.
Further information can be gathered from the difference in the relative percentages of various tissue components. It is not only the volume threshold that can trigger plaque rupture but also the relative percentage, suggesting that the biomechanical structure of plaque is fundamental. In particular, in subjects with cerebrovascular symptoms, there is an increased percentage of IPH components and lipid (also including the IPH class). Conversely, in subjects without cerebrovascular symptoms, an increased percentage of calcium and lipid-IPH was found. The protective effect of the calcium was already demonstrated by Nandalur et al,33 whereas the finding that the lipid-IPH percentage is lower in symptomatic subjects could support the histopathologic observation that lipid tissue within plaques is not active and not related to the risk of rupture.34 The ROC curve analysis confirms these results by showing the highest area under the curve with the IPH volume (AUC of 0.793, P = .001) and percentage of IPH (AUC of 0.812, P = .001). To assess the effect of some volumetric thresholds, we created 6 different models by considering the following thresholds: 10, 50, 100, 150, 200, and 250 mm3, and the best association was found by considering a threshold of 50 mm3 (P = .001, χ2 = 43.913, contingency coefficient = 0.424).
Our study has some limitations. It is a retrospective analysis, and we did not explore the association between the presence of IPH (and its volume or percentage) and the risk of new/recurrent cerebrovascular events. Instead, IPH was assessed in patients who already had cerebrovascular events, and this may have introduced a bias because some plaques may have theoretically changed in structure and composition in the interval between symptom onset and the time of CTA detection. However, we think that the limited time between the symptomatic event and the CTA reduces this potential effect. Our findings are based on a relatively small cohort, and these data will need to be validated in a larger and preferentially prospective cohort. Nevertheless, these data provide a valuable framework on which further confirmatory cohorts can be based.
Conclusions
The results of this study confirm that the value of <25 HU has a statistically significant association with the presence of cerebrovascular events and that the ratio between IPH and lipid volume represents a strong parameter for the association of cerebrovascular events.
Footnotes
The views expressed in this article are those of the author and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or US Government.
The identification of specific products or scientific instrumentation does not constitute endorsement or implied endorsement on the part of the author, Department of Defense, or any component agency.
Disclosures: Jasjit S. Suri—UNRELATED: Other: member of AtheroPoint LLC (owner). James Kevin DeMarco—UNRELATED: Grants/Grants Pending: Department of Defense*; Payment for Lectures Including Service on Speakers Bureaus: Baptist Neurological Institute, Jacksonville, Florida; Payment for Development of Educational Presentations: International Society for Magnetic Resonance in Medicine.* Waleed Brinjikji—UNRELATED: Consultancy: Superior Medical Editing (<$5000); Grants/Grants Pending: National Institutes of Health, Comments: Johnson and Johnson*; Patents (Planned, Pending or Issued): Marblehead Medical, Comments: patents pending for stroke intervention devices*; Stock/Stock Options: Marblehead Medical, Comments: cofounder of the company. *Money paid to the Institution.
References
- Received April 7, 2019.
- Accepted after revision July 15, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Carotid Plaque Calcification Attenuation Characteristics are Associated with Intraplaque Hemorrhage Volumes: A 3D Segmentation-Based Analysis
- Assessment of Attenuation in Pericarotid Fat among Patients with Carotid Plaque and Spontaneous Carotid Dissection
- Explainable machine-learning model to classify culprit calcified carotid plaque in embolic stroke of undetermined source
- Impact Analysis of Different CT Configurations of Carotid Artery Plaque Calcifications on Cerebrovascular Events
- Perivascular Fat Density and Contrast Plaque Enhancement: Does a Correlation Exist?