
Abstract
BACKGROUND AND PURPOSE: Collateral blood supply is a key determinant of outcome in large-vessel occlusion acute ischemic stroke. Single- and multiphase CTA collateral scoring systems have been described but are subjective and require training. We aimed to test whether the CTP-derived hypoperfusion intensity ratio is associated with CTA collateral status and whether a threshold hypoperfusion intensity ratio exists that predicts poor CTA collaterals.
MATERIALS AND METHODS: Imaging and clinical data of consecutive patients with large-vessel occlusion acute ischemic stroke were retrospectively reviewed. Single-phase CTA and multiphase CTA scoring were performed by 2 blinded neuroradiologists using the Tan, Maas, and Calgary/Menon methods. CTP was processed using RApid processing of PerfusIon and Diffusion software (RAPID). Hypoperfusion intensity ratio = ratio of brain volume with time-to-maximum >10 seconds over time-to-maximum >6-second volume. Correlation between the hypoperfusion intensity ratio and CTA collateral scores was calculated using the Pearson correlation. The optimal threshold of the hypoperfusion intensity ratio for predicting poor collaterals was determined using receiver operating characteristic curve analysis.
RESULTS: Fifty-two patients with large-vessel occlusion acute ischemic stroke were included. Multiphase CTA collateral scoring showed better interrater agreement (κ = 0.813) than single-phase CTA (Tan, κ = 0.587; Maas, κ = 0.273). The hypoperfusion intensity ratio correlated with CTA collateral scores (multiphase CTA: r = −0.55; 95% CI, −0.67 to −0.40; P ≤ .001). The optimal threshold for predicting poor multiphase CTA collateral status was a hypoperfusion intensity ratio of >0.45 (sensitivity = 78%; specificity = 76%; area under the curve = 0.86). Patients with high hypoperfusion intensity ratio/poor collateral status had lower ASPECTS/larger infarcts, higher NIHSS scores, and larger hypoperfused volumes.
CONCLUSIONS: The hypoperfusion intensity ratio is associated with CTA collateral status in patients with large-vessel occlusion acute ischemic stroke. The hypoperfusion intensity ratio is an automated and quantitative alternative to CTA collateral scoring methods for both clinical and future stroke trial settings.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- DCA
- diagnostic cerebral angiography
- EVT
- endovascular thrombectomy
- HIR
- hypoperfusion intensity ratio
- IQR
- interquartile range
- LVO
- large-vessel occlusion
- mCTA
- multiphase CTA
- rCBF
- relative cerebral blood flow
- ROC
- receiver operating characteristic
- sCTA
- single-phase CTA
- Tmax
- time-to-maximum
Endovascular thrombectomy (EVT) is the standard of care for eligible patients with large-vessel occlusion (LVO) acute ischemic stroke (AIS) up to 24 hours from symptom onset.1⇓⇓-4 During LVO AIS, brain tissue in the territory of an acute LVO progresses with time through varying states of ischemia (penumbra) to infarction if untreated, with retrograde leptomeningeal collateral flow supplying the ischemic brain tissue (penumbra) beyond the LVO. The quality of collateral blood supply to the affected hemisphere in LVO AIS is a significant predictor of infarct size and growth, patient functional outcome,5,6 and the rate of hemorrhagic transformation.7⇓-9 As a result, collateral status may impact eligibility for EVT as well as appropriateness for patient transfer to an EVT-capable hospital.10,11
Currently, imaging triage of collateral status is most commonly performed using CTA, and several CTA scoring systems have been devised. The Tan and Maas scoring systems were designed to evaluate collaterals on single-phase CTA (sCTA).12⇓-14 Multiphase CTA (mCTA), which includes additional late arterial and late venous phase CTAs, is the most widely studied and validated.15 The Calgary/Menon mCTA scoring system takes into account delayed filling of the MCA territory, which may be seen only in the late arterial or late venous phases. A limitation of these visual scoring systems, however, is their reliance on qualitative assessment, resulting in the need for additional training, susceptibility to reader bias, and interrater variability.16
CTP is a widely used neuroimaging technique in the work-up of LVO AIS. Maps derived from CTP can be used to estimate the size of established infarct core relative to the volume of hypoperfused brain at risk of infarction (commonly referred to as penumbra).17,18 Measuring infarct core volume and penumbra from sCTA or mCTA techniques is limited by temporal resolution. CTP acquisitions track the contrast density–bolus time curve for 45–60 seconds versus only 1–3 acquisition time points of sCTA or mCTA.
The time for brain tissue to progress from ischemic penumbra to irreversibly infarcted core varies. Collateral status is the main determinant of how quickly the penumbral tissue will progress to irreversible infarct core. This progression can happen within an hour in some patients and in others it can take >24 hours because collateral status varies from patient to patient, as well as with changes in cerebral perfusion pressure during work-up, transfer, and treatment (eg, induction/intubation) of the patient. Obtaining a quantitative measure of collateral status from the CTP acquisition may obviate the need to measure it from a CTA (single-phase or multiphase) and help prognosticate the rate of progression of the penumbral volume to irreversible infarction.
The hypoperfusion intensity ratio (HIR), defined as the ratio of the volume of tissue with a time-to-maximum (Tmax) of >10 seconds divided by the volume of tissue with a Tmax of >6 seconds,19 can be quantitatively derived from CT perfusion datasets. The HIR is a potential objective measure of collateral status19 and may be a surrogate for CTA scoring methods. This has been supported in post hoc analyses of small subcohorts of large randomized controlled trials primarily aimed at assessment of the effectiveness of EVT.20,21 Recently, for M1 segment MCA occlusions, the HIR was found to correlate well with collateral scoring using the criterion standard diagnostic cerebral angiography (DCA) scoring (American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology method) at the time of EVT.22,23
The purpose of this study was to assess whether the HIR correlates with sCTA and mCTA collateral status in patients presenting acutely with anterior circulation LVO AIS. We also aimed to determine whether a threshold HIR exists to indicate good-versus-poor mCTA collateral status.
MATERIALS AND METHODS
The study protocol was approved by the University of British Columbia institutional review board. Informed consent was waived due to the observational and retrospective analysis of anonymized data, acquired prospectively as part of routine clinical care at our institution.
Patient Population
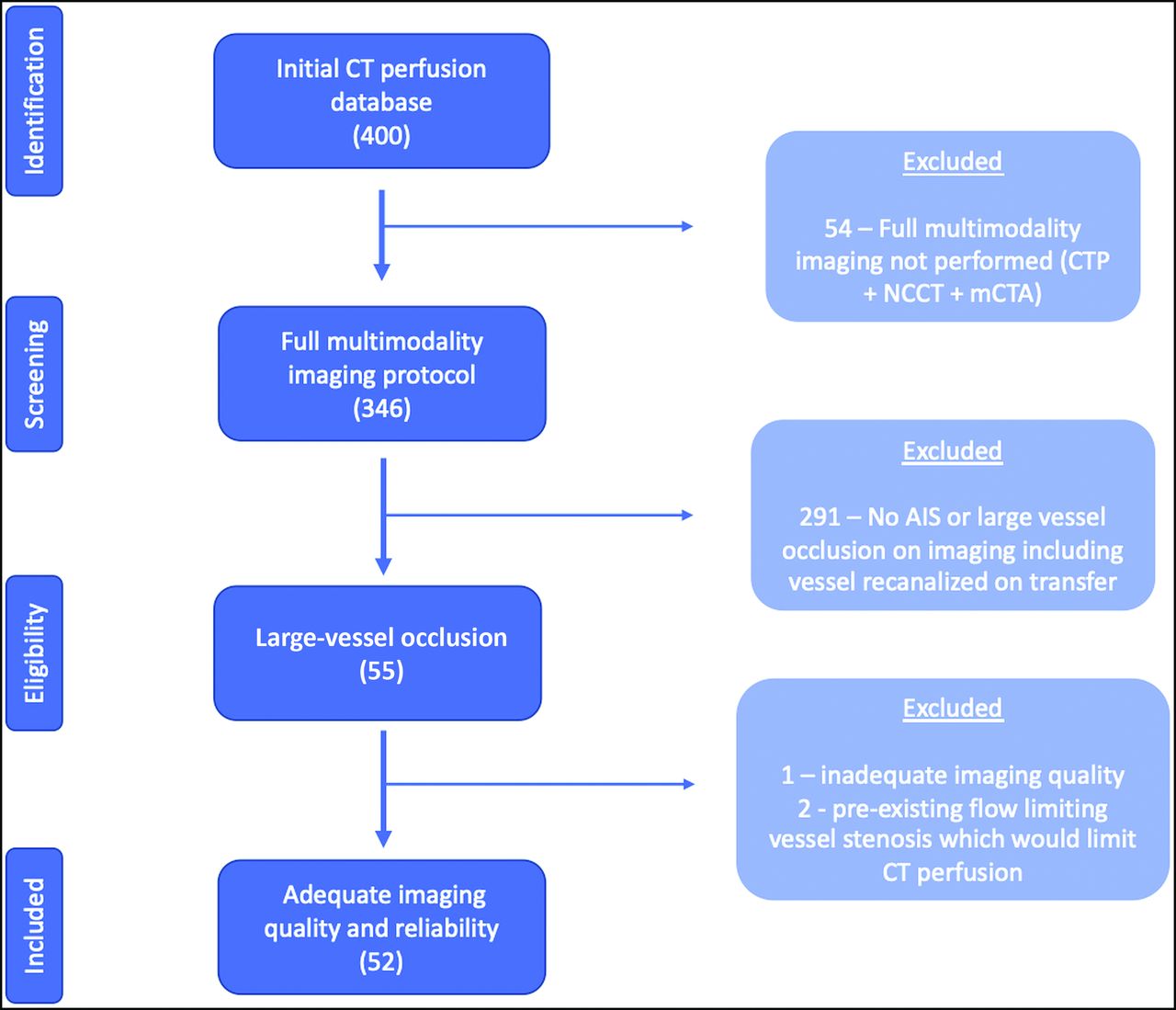
We retrospectively identified patients presenting to our comprehensive stroke center between March and September 2019 with anterior circulation LVO AIS. Most patients presenting to our institution with suspected LVO AIS during this time period were imaged with NCCT of the head, mCTA, and CTP acquired before consideration for EVT. Inclusion criteria for patients in this study were the following: 1) NCCT, mCTA, and CTP, and 2) presenting with an acute neurologic deficit due to anterior circulation LVO (ICA terminus and M1 segment MCA). We excluded patients with LVO in other locations. Isolated occlusions of the distal MCA segments (M2 and M3) also have a less clear effect on collateral blood supply, given that part of the MCA territory remains perfused via anterograde flow from other MCA branches rather than via anterior cerebral artery–MCA or posterior cerebral artery–MCA retrograde collaterals. Isolated occlusions of the anterior cerebral artery or posterior circulation were not included because they may also differ physiologically and most data regarding CTA collateral scoring methods pertain to MCA and ICA terminus occlusions.12 Additional exclusion criteria were the following: 1) poor image quality due to patient motion, significant foreign body artifacts, or inadequate acquisition; 2) pre-existing flow-limiting arterial stenosis or occlusion in the head or neck; and 3) patients in whom CT perfusion analysis failed (Fig 1).

Flow chart of patient selection.
Clinical and technical data were collected from the patient's medical records and a prospectively maintained institutional stroke data base, including age, sex, the presence of stroke risk factors, the interval between symptom onset and neuroimaging, the initial NIHSS score, and the use of intravenous tPA (alteplase).
Imaging Protocol and Imaging Reconstruction
Images were acquired using a standardized institutional acute stroke protocol (Online Supplemental Data) on 1 of 3 CT scanners at our institution: a 192-section multidetector dual-source scanner (Somatom Force; Siemens) and 1 of two 128-section multidetector dual-source scanners (Definition Flash; Siemens).
Single-phase and multiphase CTAs were reconstructed at the CT acquisition workstation running Somatom Somari 7 (Siemens). Time-density curves for the input artery and output vein were automatically obtained from the contralateral ICA and superior sagittal sinus, respectively; then perfusion maps were automatically derived using automated RApid processing of PerfusIon and Diffusion software (RAPID; ISchemaView). Infarct core volume was defined as the volume of tissue with a cerebral blood flow of <30% relative to the unaffected hemisphere on CTP (relative CBF [rCBF] <30%). Hypoperfusion volumes were quantitatively measured by the perfusion delay on the Tmax maps. HIR was defined as the ratio of the Tmax >10-second lesion volume divided by the Tmax >6-second lesion volume.20 Mismatch volume (reflecting the hypoperfused penumbra around the infarct core) was defined as the Tmax >6-second volume minus the rCBF <30% volume. No manual correction of processed CTP images was performed.
Imaging Analysis
CTA collateral scoring was performed by 2 fellowship-trained diagnostic neuroradiologists, each with 5 years of experience, both blinded to clinical information and CTP output (including the HIR). Previously validated scoring systems were used, designed to assess collateral status on sCTA (Tan et al,13 and Maas et al14), and mCTA (Calgary/Menon scoring system),15 respectively. Correlation with DCA collateral status was not performed because DCA collateral scoring methods are limited to M1 occlusions, and not all patients were taken to angiography and thrombectomy. For sCTA collateral scoring methods, the initial (early arterial) phase of mCTA was used.
The Tan scoring system is a 4-point scale for sCTA: grade 0, zero collateral filling in the affected territory; grade I, filling in the affected territory, <50% of the contralateral side; grade II, filling >50% but <100% than in contralateral territory; grade III, filling equal to the contralateral territory. The Maas scoring system is a 5-point scale for sCTA: grade I, zero filling in the affected territory; grade II, filling less in the affected territory than in the contralateral territory; grade III, filling equal to the contralateral territory; grade IV, filling greater than in the contralateral territory; and grade V, exuberant filling in the affected territory. The Calgary/Menon scoring system is a 6-point scale for mCTA: grade 0, zero filling in any phase in the affected territory; grade I, just a few vessels visible in any phase; grade II, delay of 2 phases and decreased prominence or number of vessels, or delay of 1 phase and some ischemic areas with no vessels; grade III, delay of 2 phases but the same prominence or number of vessels, or delay of 1 phase with the prominence or number of vessels significantly decreased; grade IV, delay of 1 phase but prominence and extent are the same; and grade V, no delay and normal or increased number or prominence of vessels.
Statistical Analysis
Nominal variables were summarized using frequency descriptive analysis and then compared using the Fisher exact test. Continuous variables were assessed for normality using histogram analysis and then summarized using mean (SD), median, and interquartile range (IQR) as appropriate and then tested using the Mann-Whitney U test. The sCTA and mCTA scores calculated by each of the 2 raters were tested for interrater reliability using square-weighted κ analysis (Cohen κ).24 Patients were then dichotomized into 2 subgroups on the basis of collateral score of good and poor collaterals as follows: Tan sCTA score, 2–3 = good, 0–1 = poor;13 Maas sCTA score, 3–5 = good, 1–2 = poor;14 Calgary/Menon mCTA score, 4–5 = good, 0–3 = poor.25 Univariate analysis was performed to compare initial stroke severity assessed by the NIHSS score, core infarct volume, Tmax volumes, mismatch volume, and perfusion mismatch ratio between good and poor mCTA collateral groups using the Mann-Whitney U test. The correlations between the HIR and the CTA collateral scores were calculated using the Pearson correlation. Receiver operating characteristic (ROC) curve analysis was performed to assess the diagnostic performance of the HIR in predicting poor mCTA collateral status (scores of 0–3). The Youden index was used to determine the optimal threshold HIR from the ROC curve for predicting poor mCTA collateral status. The corresponding specificity and sensitivity of the optimal HIR thresholds for poor-versus-good CTA collateral status were also calculated. Similarly, ROC curve analyses determining of the optimal HIR thresholds for predicting poor-versus-good Tan sCTA collateral status (scores of 0–1) and poor Maas sCTA collateral status (scores of 1–2), and specificity and sensitivity of the optimal HIR thresholds were also performed.
Statistical analysis was performed using the R statistical and computing software (http://www.r-project.org/) and SPSS Statistics, Version 24 (IBM). Statistical tests were considered significant at a P value < .05.
RESULTS
Patient Population
Between March and September 2019, four hundred patients were assessed with multimodality neuroimaging for suspected AIS, including mCTA and CTP at our center. A total of 52 patients were included in this study (Fig 1). There were no significant differences in the age, sex, or vascular risk factors between the groups with good and poor mCTA collaterals (Table 1).
Baseline characteristics for all patients according to Calgary/Menon mCTA collateral scale
There was no significant difference in the location (ICA versus M1) of the LVO between groups with good and poor collateral status (P = .97) and no difference in the laterality of the LVO between groups (P = .26). The median NIHSS at presentation was lower in those with good collateral scores (15; IQR = 8–19) versus poor scores (19; IQR = 14–21; P = .05). The median ASPECTS was 7 (IQR = 5–8) for all patients, with a higher baseline ASPECTS seen in patients with good collaterals on mCTA (P = .003).
The median time between symptom onset and CT/CTA/CTP was significantly longer in the group with good mCTA collaterals (median, 374 minutes; IQR = 191–598 minutes) versus poor collaterals (median, 116 minutes; IQR = 67–285 minutes). The time from last known well to administration of IV tPA was not significantly different between groups.
Image Analysis
Interrater agreement was excellent when using the Calgary/Menon mCTA scoring method (κ = 0.813), moderate using the Tan sCTA scoring method κ = 0.587), and fair using the Maas sCTA scoring method (κ = 0.273).24
Calgary/Menon mCTA Scores.
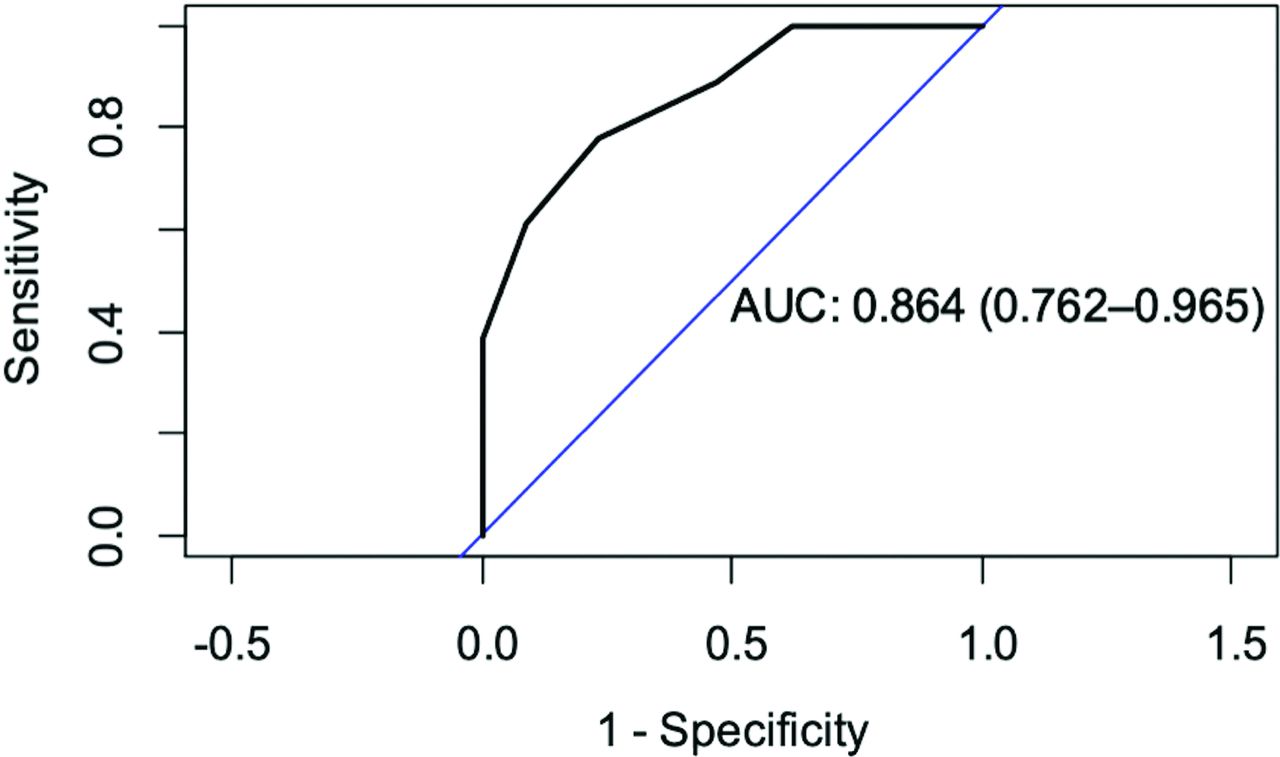
The HIR was significantly greater in those with poor-versus-good mCTA collateral scores (HIR = 0.60; IQR = 0.40–0.70 versus 0.30; IQR = 0.10–0.45; P ≤ .001) (Table 2). The HIR showed a strong correlation with Calgary/Menon mCTA scores (Pearson correlation coefficient = −0.55; 95% CI, −0.67 to −0.40; P ≤ .001). ROC curve analysis showed a significant association between poor collaterals and the HIR (P ≤ .001) with an area under the curve of 0.86. The optimal HIR threshold for prediction of poor-versus-good mCTA collateral status (scores of 0–3) was 0.45 (specificity = 76%, sensitivity = 78%) (Fig 2).

ROC analysis of the HIR to predict poor collaterals (Calgary/Menon mCTA scores 0–3) with an area under curve (AUC) of 0.864. An HIR of 0.45 was the optimal threshold that predicted poor-versus-good mCTA collaterals, with sensitivity = 78%, specificity = 76%.
HIR, rCBF <30%, and Tmax volumes depending on collateral score using the Calgary/Menon method
Tan sCTA Scores.
HIR ratios were significantly greater in those with poor-versus-good Tan sCTA collateral scores (HIR = 0.60; IQR = 0.50–0.80 versus 0.30; IQR = 0.15–0.50; P < .001) (Online Supplemental Data). The HIR showed a strong correlation with Tan sCTA scores (Pearson correlation coefficient = −0.54; 95% CI, −0.67 to −0.39; P < .001). ROC curve analysis showed a significant association between poor collaterals and HIR (P< .001), with an area under the curve of 0.87. The optimal HIR threshold for prediction of good-versus-poor collateral status was 0.55 (specificity = 89%, sensitivity = 67%).
Maas sCTA Scores.
HIR ratios were significantly greater in those with poor-versus-good Maas sCTA collateral scores (HIR = 0.50; IQR = 0.4–0.6 versus 0.20; IQR = 0.05–0.40); P <.001) (Online Supplemental Data). The HIR showed a strong correlation with Maas sCTA scores (Pearson correlation coefficient = −0.38; 95% CI, −0.53 to −0.20; P < .001). ROC curve analysis showed a significant association between poor collaterals and HIR (P < .001) with an area under the curve of 0.82. The optimal HIR threshold for prediction of good-versus-poor collateral status was 0.25 (specificity = 55%, sensitivity = 94%).
DISCUSSION
In this study, CTP-derived HIR correlated well with sCTA and mCTA collateral scoring methods. In addition, this study identified an HIR threshold of >0.45 as an optimal predictor of poor collateral status on mCTA and demonstrated a significant association between favorable collaterals and a better baseline imaging profile (smaller penumbra/hypoperfused volume and infarct core volumes).20,23 This study is the first primary analysis comparing the HIR with several CTA collateral scoring methods in the setting of anterior circulation LVO AIS. Our study population included patients from both the early and late windows and supports the use of the HIR in assessing collateral status.26 For institutions routinely performing CTP with appropriate postprocessing software for LVO AIS work-up, the capability of CTP to assess collaterals in addition to mapping mismatch between infarct volume and penumbra may obviate the need for multiphase CTA for collateral assessment, despite the slight increase in radiation dose. In addition, poor interrater agreement was observed in this study for sCTA collateral scoring methods (Tan and Maas), suggesting that sCTA alone for collateral assessment is suboptimal.
The ability to automatically derive an objective measure of collateral status using CTP may have important clinical implications for triage and decision-making for EVT. The HIR is a measure of collateral blood flow within ischemic brain tissue using CT or MR perfusion imaging.12,15,20 Traditionally, non-invasive evaluation of collateral status in LVO AIS has focused primarily on CTA techniques. Several scales have been developed for assessing collateral status on CTA on the basis of the degree of contrast opacification of the MCA branches distal to the occlusion.17,18,27
There may be significant advantages in using the HIR for collateral assessment compared with these CTA visual scoring systems. The HIR is a quantitative assessment, requiring no additional training for scoring scales (Fig 3), thereby eliminating susceptibility to reader bias and interrater variability (the latter particularly pronounced for sCTA methods in this study). Although the interrater agreement for mCTA scores in this study was high and in keeping with other mCTA studies, this finding is based on data generated by trained/experienced neuroradiologist interpretations of mCTA. A large portion of CTAs are read by non-neuroradiologists, however, and mCTA use is not widespread. In contrast, after the DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN)4 trial and the Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke (DEFUSE3)3 trial, use of CTP has grown significantly. In addition, there is recent evidence of a benefit of CTP in the first 9 hours of AIS for selecting patients with LVO as well as non-LVO to receive intravenous tPA.28

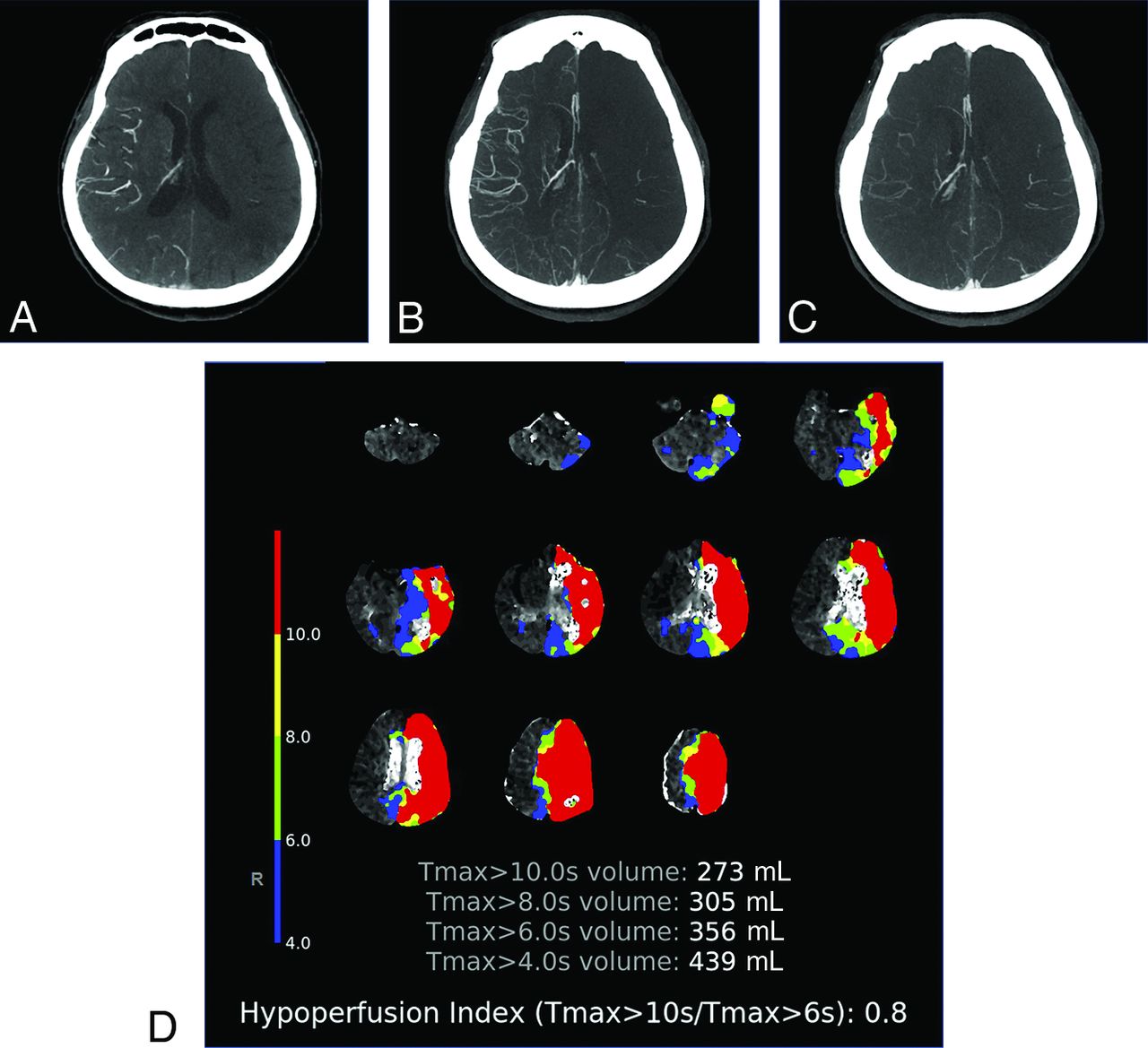
Patient with acute occlusion of the left terminal ICA and poor collateral blood supply. A–C, Multiphase CTA images show early arterial (A), late arterial (B), and late venous (C) phases, respectively, with only a small number of left MCA territory branches filling in any phase. D, HIR Color map shows color coded areas of increased Tmax in the left MCA territory with the HIR calculated as 0.8 (red = Tmax >10 seconds, yellow = >8 seconds, blue = >6 seconds, green = >4 seconds). S indicates seconds.
Because the HIR can be derived from routine CTP acquisitions, it can be quickly integrated in LVO AIS stroke imaging workflow. Moreover, commercially available software platforms that automate the derivation and reporting of the HIR may provide valuable time-savings and rapid availability of results via messaging platforms to the entire multidisciplinary stroke team, expediting the decision-making process. These features may also be particularly useful for facilitating referrals from primary stroke centers with physicians less experienced in assessing collateral status on CTA during initial stroke imaging work-up. In addition, rapid assessment of collateral status using the HIR may be also useful in “spoke” centers for selecting eligible candidates and preventing futile transfers to “hub” EVT-capable centers because patients with poor collateral status (high HIR) are less likely to undergo EVT, have higher stroke severity and infarct growth, increased risk of hemorrhagic infarct transformation, and worse functional outcomes.10,11,19,20,23,29⇓⇓-32
While CT-based AIS imaging work-up has become more widespread due to logistic and resource advantages, some centers use MR imaging. However, time-of-flight MRA in the setting of an LVO AIS does not allow evaluation of the distal vascular bed, preventing collateral assessment by MRA. In a study by Guenego et al,23 53% (52/98) of patients had MR imaging before EVT, and collateral assessment on MRA was not possible in these patients. Because the HIR can be derived from MR perfusion, centers that favor MR imaging for EVT triage may also benefit from the HIR as a measure of collateral status.
Our findings are consistent with recently reported data correlating the HIR with criterion standard DCA-derived collateral scores for patients with M1 occlusion (ICA occlusions excluded) assessed during EVT as a primary analysis23 and with CTA collateral scores as secondary analyses.15 DCA is considered the criterion standard method for dynamically assessing the cerebral arteries, yet this assessment can be derived only during EVT, which limits its utility on LVO AIS decision-making. The same study of DCA-derived collateral scores of patients with M1 occlusion found a similar cutoff of <0.4 for predicting good collateral status.23 While it is expected that the HIR would correlate with CTA collateral status because it correlates with DCA, it is important to validate it against CTA. Collateral status on DCA may differ from that on CTA, for example, if the patient's blood pressure changes due to the hypotensive effects of medications or anesthesia.
Previous studies comparing the HIR with sCTA have also reported similar findings. A post hoc analysis of a small subcohort of the Solitaire With the Intention For Thrombectomy as Primary Endovascular Treatment (SWIFT-PRIME) trial found that CTP-derived HIR correlates with sCTA-based collateral status, with good collaterals having a median HIR value of 0.4 and excellent collaterals having a median HIR value of 0.3.21 Similar post hoc analysis of the DEFUSE-3 trial found that a lower HIR correlates with slower infarct growth and smaller final infarct volume.20 These studies were, however, limited by potential selection bias as well as heterogeneous neuroimaging protocols due to their post hoc nature and large multicenter design.
This study is limited by its retrospective design, with data from a single center. We chose not to compare the HIR with DCA collateral status because it has already been shown to correlate well16 and we did not want to restrict analysis to solely M1 occlusions. We also restricted our analysis to some commonly used CTA scoring methods; however, we acknowledge that several alternative subjective CTA collateral scoring methods exist. We did not include other vessel-occlusion locations (ie, isolated M2, M3, anterior cerebral artery, posterior cerebral artery, or basilar artery occlusions). The HIR thresholds derived from this retrospective dataset need to be further validated. We also acknowledge that currently only 1 CTP processing software vendor has automated HIR output, which limits use of this technique. Further study of the correlation of the HIR with initial and final infarct volume, hemorrhagic transformation, and patient functional outcome is also warranted and may encourage additional vendors to incorporate this tool into future iterations of their software packages.
CONCLUSIONS
The HIR is associated with CTA collateral status in patients presenting with LVO AIS. As an automated and quantitative tool, it may be rapidly obtained and is easier to interpret than subjective CTA collateral scoring methods. Current clinical practice and future clinical LVO AIS trials may consider use of the HIR for assessment of patient collateral status at the time of initial stroke imaging work-up.
Footnotes
Preliminary findings previously presented at: Annual Meeting of the American Society of Neuroradiology, May 30 to June 4, 2020; Virtual.
References
- Received September 24, 2020.
- Accepted after revision February 19, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Association between intraprocedural drops in blood pressure and infarct growth rate patterns after acute large-vessel occlusions
- Hypoperfusion Intensity Ratio and Hemorrhagic Transformation in Patients with Successful Recanalization after Thrombectomy
- Perfusion Collateral Index versus Hypoperfusion Intensity Ratio in Assessment of Collaterals in Patients with Acute Ischemic Stroke
- Alberta Stroke Program Early CT Score and collateral status predict target mismatch in large vessel occlusion with delayed time windows
- Thrombectomy Outcomes With General vs Nongeneral Anesthesia: A Pooled Patient-Level Analysis From the EXTEND-IA Trials and SELECT Study
- Correlation of Collateral Scores Derived from Whole-Brain Time-Resolved Flat Panel Detector Imaging in Acute Ischemic Stroke
- RAPID CT Perfusion-Based Relative CBF Identifies Good Collateral Status Better Than Hypoperfusion Intensity Ratio, CBV-Index, and Time-to-Maximum in Anterior Circulation Stroke