
Abstract
BACKGROUND AND PURPOSE: Accurate pretreatment diagnosis and assessment of spinal vascular malformations using spinal CTA are crucial for patient prognosis, but the postprocessing reconstruction may not be able to fully depict the lesions due to the complexity inherent in spinal anatomy. Our purpose was to explore the application value of the spinal subtraction and bone background fusion CTA (SSBBF-CTA) technique in precisely depicting and localizing spinal vascular malformation lesions.
MATERIALS AND METHODS: In this retrospective study, patients (between November 2017 and November 2022) with symptoms similar to those of spinal vascular malformations were divided into diseased (group A) and nondiseased (group B) groups. All patients underwent spinal CTA using Siemens dual-source CT. Multiplanar reconstruction; routine bone subtraction, and SSBBF-CTA images were obtained using the snygo.via and ADW4.6 postprocessing reconstruction workstations. Multiple observers researched the following 3 aspects: 1) preliminary screening capability using original images with multiplanar reconstruction CTA, 2) the accuracy and stability of the SSBBF-CTA postprocessing technique, and 3) diagnostic evaluation of spinal vascular malformations using the 3 types of postprocessing images. Diagnostic performance was analyzed using receiver operating characteristic analysis, while reader or image differences were analyzed using the Wilcoxon signed-rank test or the Kruskal-Wallis rank sum test.
RESULTS: Forty-nine patients (groups A and B: 22 and 27 patients; mean ages, 44.0 [SD, 14.3] years and 44.6 [SD,15.2] years; 13 and 16 men) were evaluated. Junior physicians showed lower diagnostic accuracy and sensitivity using multiplanar reconstruction CTA (85.7% and 77.3%) than senior physicians (93.9% and 90.9%, 98% and 95.5%). Short-term trained juniors achieved SSBBF-CTA image accuracy similar to that of experienced physicians (P > .05). In terms of the visualization and localization of spinal vascular malformation lesions (nidus/fistula, feeding artery, and drainage vein), both multiplanar reconstruction and SSBBF-CTA outperformed routine bone subtraction CTA (P = .000). Compared with multiplanar reconstruction, SSBBF-CTA allowed less experienced physicians to achieve superior diagnostic capabilities (comparable with those of experienced radiologists) more rapidly (P < .05).
CONCLUSIONS: The SSBBF-CTA technique exhibited excellent reproducibility and enabled accurate pretreatment diagnosis and assessment of spinal vascular malformations with high diagnostic efficiency, particularly for junior radiologists.
ABBREVIATIONS:
- AP
- arterial phase
- AUC
- area under the curve
- CE-MRA
- contrast-enhanced MRA
- MPR-CTA
- multiplanar reconstruction CTA
- RBS-CTA
- routine bone subtraction CTA
- ROC
- receiver operating characteristic
- SSBBF-CTA
- spinal subtraction and bone background fusion CTA
- SVM
- spinal vascular malformation; 3D-VR =3D volume-rendering
Spinal vascular malformations (SVMs) are rare CNS vascular lesions, with spinal AVFs (arteriovenous directly shunting with a fistula) and AVMs (arteriovenous connection with a true nidus) being the most common types (95%).1 Their clinical presentations are variable and nonspecific, including progressive motor, sensory, and urogenital disturbances, similar to chronic myelitis, demyelinating lesions, disc lesions, and so forth.2,3 However, the treatments and prognoses differ completely. Delayed or incorrect diagnosis and treatment can lead to serious complications, permanent disability, and even fatality.4⇓-6 Therefore, accurate diagnosis and evaluation before treatment are crucial for developing an appropriate treatment plan and improving neurologic function.
Spinal DSA is the criterion standard for diagnosing SVMs.7,8 However, selective level-by-level radicular spinal DSA is technically difficult, particularly in patients with atherosclerosis or vascular variations. This not only consumes time with an increased incidence rate of neurologic complications but also results in a high burden of iodinated contrast and radiation exposure.7,9,10 Therefore, pre-DSA noninvasive vascular imaging examinations, such as CTA or contrast-enhanced MRA (CE-MRA), are crucial for the preliminary diagnosis and angioarchitecture evaluation of SVMs.11⇓-13 These insights can aid clinicians in optimal preoperative preparation, potentially reducing the operative duration and elevating surgical outcomes.14,15
Despite being radiation-free and having high tissue resolution, the use of CE-MRA for preoperative assessment is still limited because of the long scanning time, small scanning range per scan, and large contrast agent dosage, which can make it difficult for patients to remain motionless for protracted periods.9,16 However, CTA can effectively address these issues, on the basis of its advantages of fast scanning speed for obtaining the entire range of the spine in a short time and high spatial resolution for displaying smaller subcortical blood vessels.12 The advantages of CTA are yet to be explored further, especially in the area of vascular image postprocessing. Difficulty in simultaneous and clear display of the vertebral body and abnormal small blood vessels within the vertebral canal is the limitation of routine 3D volume rendering (3D-VR) reconstruction for SVMs.12 On the basis of extensive clinical experience, even with meticulous bone subtraction techniques, the 3D-VR reconstruction images still have difficulty presenting the core lesions of SVMs, much less achieving a comprehensive representation of the extensively draining venous network.
This study proposes an improved 3D-VR technique, the spinal subtraction and bone background fusion CTA (SSBBF-CTA) technique, which obviates the requirement for third-party software integration. It optimizes the display of angioarchitectures of lesions and their relationship with the bones. The use of SSBBF-CTA for the accurate diagnosis and localization of SVMs can substantially assist in preoperative evaluation and clinical treatment decisions.
MATERIALS AND METHODS
Patients
Forty-nine patients, including 22 patients diagnosed with SVMs (group A) and 27 patients without SVMs (group B), between November 2017 and November 2022, were retrospectively enrolled in our study. The inclusion criteria were as follows: 1) clinical manifestations of motor/sensory disturbances; 2) all patients having undergone spinal CTA examinations, including precontrast and arterial phase (AP) imaging; 3) group A: DSA examination conducted within 1 week that confirmed the diagnosis of SVMs; and 4) group B: DSA, MR imaging, and other sufficient evidence that confirmed the absence of SVMs by clinical physicians and radiologists with >10 years of experience. The exclusion criteria were as follows: 1) insufficient or incomplete clinical data, 2) intramedullary tumors or after aortic replacement surgery, and 3) severe motion artifacts on images. The patient screening process is illustrated in the flow chart shown in Fig 1. This retrospective study received approval from the institutional review board and was granted an exemption from the requirement for informed consent.

Flow chart of the patient enrollment process and workflow of this study. Asterisk indicates accurate localization of critical lesions which defined as mostly correct when multiple feeding arteries are present, and the identification of drainage veins covering over 70% of the range.
CT Protocol
All patients underwent multiphasic CT consisting of precontrast and AP images using a Somatom Definition Flash CT scanner (Siemens). The scan parameters were as follows: 10-0kV tube voltage, tube current determined by the Automatic Tube Current Modulation system (Care Dose4D, Siemens; 100-mAs reference tube current, and 120- to 350-mAs effective tube current), 0.28-second gantry rotation time, 1.2 pitch, 64 × 0.6 mm collimation. All data sets were reconstructed with a slice thickness of 0.75 mm and an increment of 0.5 mm. The contrast agent (iomeprol, Iomeron, 400 mgI/mL; Shanghai Bracco Sine Pharmaceutical) was injected at a flow rate of 0.075 mL/kg/s, 14-second injection duration, and 10-second same flow of saline. The AP determined by the bolus-tracking technique started 8 seconds after the threshold of the ascending aorta reached 120 HU. The scanning ranges of the 2 phases were identical.
Image Postprocessing
First, all the original images, including the precontrast and AP images, were transferred to a postprocessing workstation (syngo.via VB20; Siemens), and the multiplanar reconstruction images were obtained. Routine bone subtraction CTA (RBS-CTA) 3D-VR images were obtained by subtracting the precontrast images from the AP images on the basis of the currently more precise bone subtraction algorithm of Siemens. Second, all original and RBS-CTA images were transferred to the ADW4.6 workstation (GE Healthcare), which is more proficient in the reconstruction of microvascular structures. Bone background images were obtained by reconstructing precontrast images. The aortic trunk and branches were obtained from the RBS-CTA images. Abnormal vascular structures were identified by processing the original AP images. The fusion of the 3 aforementioned types of images produced SSBBF-CTA images. The MPR images were postprocessed in real-time following patient scanning, whereas the RBS and SSBBF-CTA images were processed retrospectively.
Image Analysis and Evaluation Criteria
Three major steps were involved in image analysis. Patients were randomly assigned to each reading session. All readers read the images independently and blinded to the final diagnosis. Postprocessing image reconstruction and diagnostic accuracy were evaluated against DSA as the criterion standard, which was verified by seasoned vascular interventionalists (Online Supplemental Data).
1) Preliminary screening capability using original images with MPR-CTA to evaluate the actual diagnostic accuracy of SVMs when radiologists first read radiographs using only general images. The patients in groups A and B were randomized, and 3 types of readers 1–3 participated in this step. Reader 1 was a junior undergoing radiologist training with 1 year of experience. Reader 2 was a type of junior practicing radiologist with 3–8 years of experience, who submitted the original diagnostic report for the first time. Reader 3 was a type of senior radiologist with >10 years of experience who signed the report.
2) The accuracy and stability of the SSBBF-CTA postprocessing technique to evaluate whether the postprocessing method of SSBBF-CTA performed by radiologists with different experience levels was accurate and repeatable. Images of group A were used. The SSBBF-CTA image postprocessing was performed by 2 practicing radiologists with 4 and 20 years of experience (readers 4 and 5, respectively), and the differences between the 2 were assessed. The classification criteria (types 1–4) of SSBBF-CTA images are shown in Fig 1, including the localization and number of nidus/fistulas and feeding arteries, the extent of the drainage vein, and overall morphology.
3) Diagnostic value of lesion details of SVMs using 3 types of postprocessing images to analyze the lesion details (visualization and localization of feeding arteries, nidus/fistula, and draining veins) by different 3D-VR images and compare the differences among the 3. Reader 1 (same as above) and reader 4 evaluated and scored the lesions of SVMs in the MPR-CTA, RBS-CTA, and SSBBF-CTA images, respectively. All final scores were confirmed by discussion in cases of disagreement and supervised by reader 5. Finally, a comparison of the diagnostic time was made between reader 1 and reader 4 in terms of evaluating all SVM lesions using MPR-CTA and SSBBF-CTA. The scoring criteria for the visualization/localization of lesions (evaluating feeding arteries, nidus, and draining veins separately) and overall morphology in MPR, RBS, and SSBBF-CTA images are shown in Fig 1.
Statistical Analysis
Demographic and clinical variables were compared between patients in groups A and B. The Mann-Whitney U test was used for non-normally distributed quantitative data. For normally distributed data, the independent samples t test was used. χ2 tests were performed on categoric data. Receiver operating characteristic (ROC) analysis was performed to evaluate the diagnostic performance of readers 1–3, using DSA diagnosis as the criterion standard. Comparison of the areas under the ROC curves was performed using the DeLong test. The Wilcoxon signed-rank test was used to compare the differences between the postprocessed images of readers 4 and 5, as well as the differences in diagnostic evaluation and time between readers 1 and 4. The Kruskal-Wallis rank sum test was used to compare the differences in lesion identification and localization among the different postprocessing images.
All continuous variables were expressed as mean (SD) when normally distributed and median (interquartile range) if not. Statistical significance was set at P < .05. Statistical analyses were performed using SPSS (Version 25.0; IBM) and MedCalc (Version 18.21.1; MedCalc Software).
RESULTS
Patient Characteristics
Of 63 patients with similar symptoms of spinal cord compression who underwent preoperative spinal CTA, 14 were excluded from this study for the following reasons: 1) insufficient clinical data (n = 3); 2) patients with intramedullary tumors (n = 1) or aortic replacement surgery (n = 1); 3) images with severe motion artifacts (n = 1); 4) patients suspected of having SVMs without confirmed DSA (n = 3); and 5) no sufficient evidence to exclude patients with SVMs (n = 5). Accordingly, 49 patients (group A: 22 patients; mean age, 44.0 [SD, 14.3] years; and group B: 27 patients; mean age 44.6 [SD, 15.2] years) comprised the final study sample, and their demographic and clinical variables are summarized in Table 1. Only urogenital disturbances showed statistically significant differences between patients with and without SVMs (P = .005).
Patient characteristicsa
Preliminary Screening of SVMs
The diagnostic efficacies of the original images with MPR for the primary screening of SVMs by different readers are shown in Table 2. As radiologic experience increased, the area under the curve (AUC) values for readers 1, 2, and 3 were 0.849, 0.936, and 0.977, respectively. Among all diagnostic indicators, sensitivity was the least effective, with reader 1 demonstrating a sensitivity of only 77.3%. Moreover, the DeLong test demonstrated a statistically significant difference between the ROC curves of reader 1 and reader 3 (P = .031).
Diagnostic efficacy of original images with MPR for primary screening of SVMs by different readersa
SSBBF-CTA Postprocessing Images
The SSBBF-CTA images processed by readers 4 and 5 were classified into 4 types: types 1–4. The higher the classification level, the greater was the clinical utility, with types 3 and 4 being considered particularly beneficial in aiding clinical diagnosis and treatment. Nearly all lesion characteristics, including localization and the number of nidi/fistulas, drainage veins, and overall morphology, were classified as either type 3 or 4, with the majority falling into the type 4 category (Fig 2). Only 2 cases had deviations in the feeding artery, characterized by the presence of multiple supplying vessels or the involvement of complex scenarios involving the extracranial arteries and intracranial collateral circulation (Online Videos 1 and 2). In addition, no statistically significant difference was observed between readers 4 and 5 (P > .05).

Percentage of stacked bar chart of categorization of postprocessing SSBBF reconstruction accuracy. Types 3 and 4 are considered particularly beneficial in aiding clinical diagnosis and treatment.
Diagnosis and Evaluation of SVMs Using Different CTA Postprocessing Images
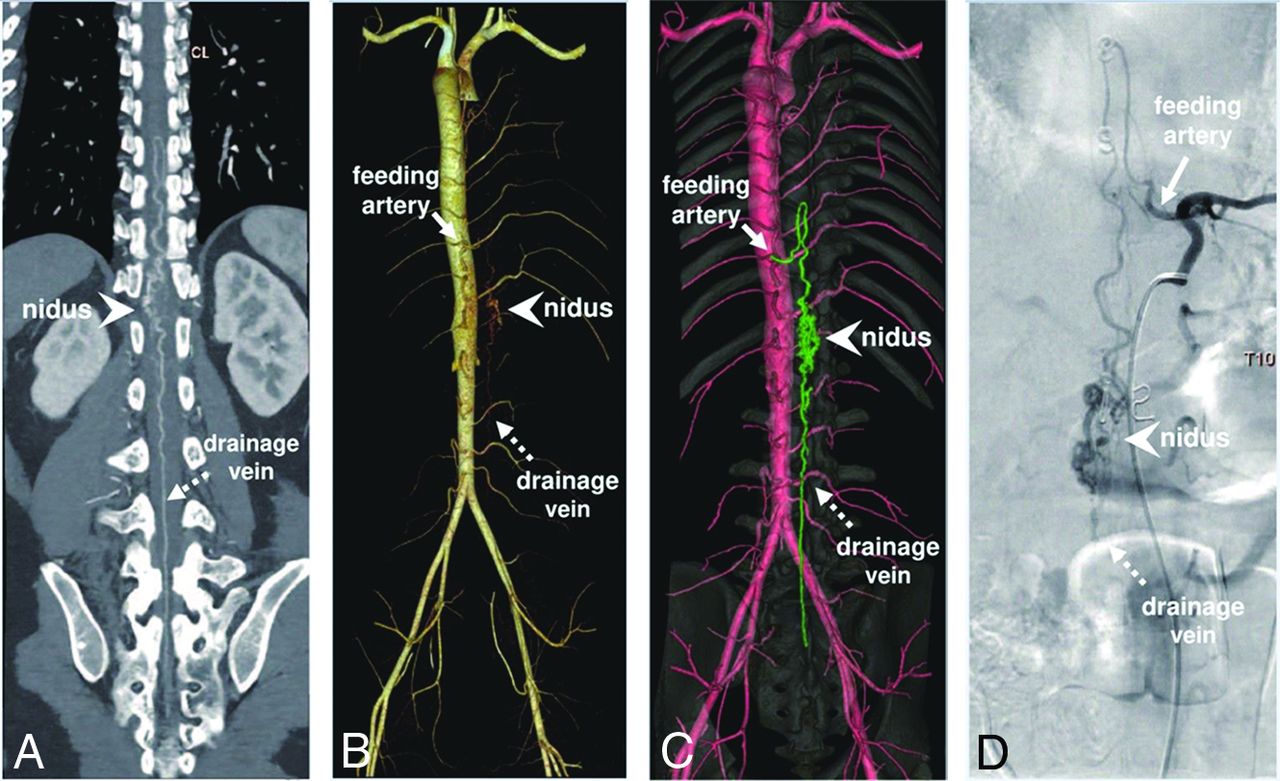
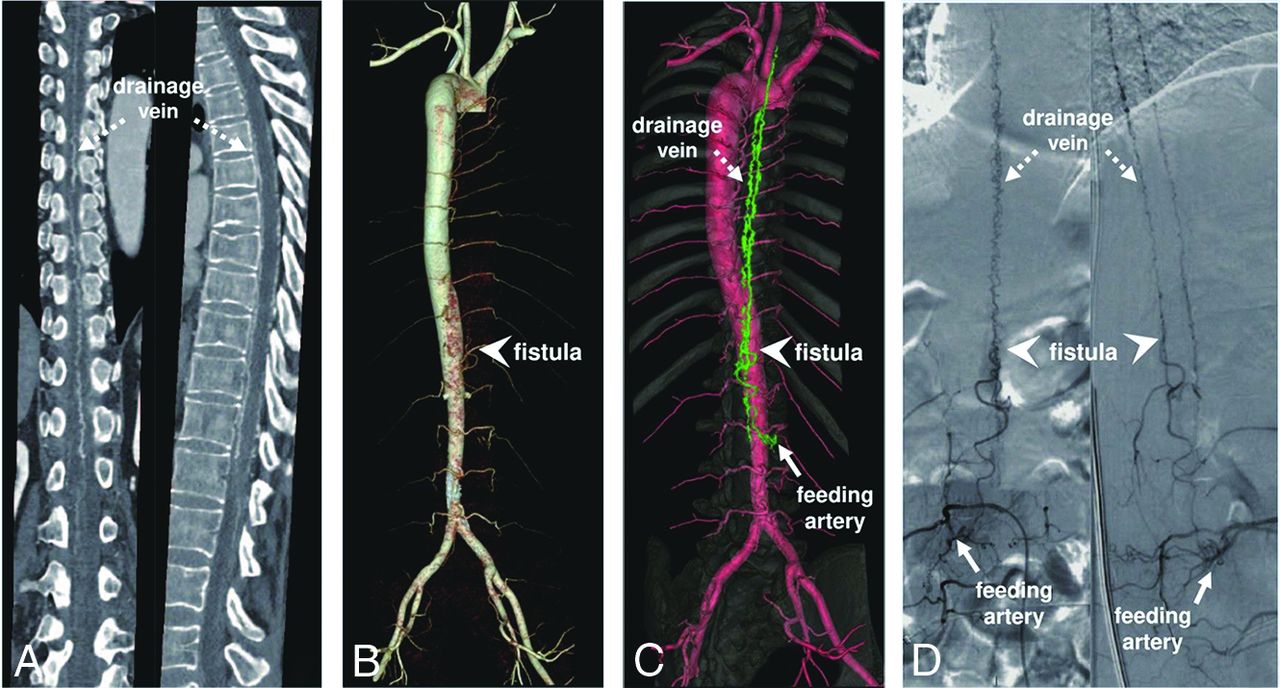
We compared the diagnostic capabilities of SVM lesions using 3 postprocessing methods (MPR-CTA, RBS-CTA, and SSBBF-CTA, Figs 3 and 4, Online Videos 3 and 4), using scores that were discussed by readers 1 and 4 and subsequently corrected under the supervision of reader 5. In terms of accuracy in visualization and localization of lesions (nidus/fistula, feeding artery, and drainage vein) and the overall morphology of SVMs, RBS-CTA demonstrated significantly inferior performance (P = .000) compared with MPR-CTA and SSBBF-CTA, whereas no significant difference (P >.05) was observed between MPR and SSBBF (Table 3). Additionally, reader 1 performed worse than reader 4 in the assessment of lesions using MPR-CTA (P < .05), whereas no difference (P >.05) was observed between the 2 when using SSBBF-CTA (Table 4 and Online Supplemental Data). Moreover, both readers 1 and 4 required significantly less diagnostic time when using SSBBF-CTA for lesion assessment than when using MPR-CTA (P = .000, Table 4).

Spinal CTA images in a 28-year-old man with a spinal AVM. The crucial lesions, including nidus (arrowhead), feeding artery (solid arrow), and drainage vein (dotted arrow), are shown in MPR-CTA (A), RBS-CTA (B), SSBBF-CTA (C), and DSA images (D).

Spinal CTA images in a 55-year-old woman with a spinal AVF. The crucial lesions, including the fistula (arrowhead), feeding artery (solid arrow), and drainage vein (dotted arrow), are shown in an MPR-CTA image (A), a RBS-CTA image (B), SSBBF-CTA image (C), and a DSA image (D).
Scoring of lesion localization and visualization of SVMs using different postprocessing techniques of CTA imagesa
Assessment of lesions of SVMs and diagnostic time using different postprocessing CTA techniques by different readersa
DISCUSSION
This study used clinically prevalent postprocessing workstations to optimize postprocessing techniques for spinal artery CTA, achieving precise visualization and localization of SVM lesions using 3D-VR, thereby enhancing the diagnostic ability and efficiency of radiologists. This advancement allows clear visualization of tertiary and higher-order arterial branches within 3D-VR images, potentially having considerable importance for the diagnostic utility of CTA in vasculopathy.
The accuracy of SVM diagnosis using the original and MPR-CTA images was lower for junior physicians than for more experienced physicians, particularly in terms of diagnostic sensitivity. The incidence rate of SVMs was quite low, making it impractical to reach an occurrence rate of approximately 50% in this study. Therefore, in the practical field of radiology, the likelihood of diagnostic errors or missed diagnoses is even higher.17 However, the consequences of a missed diagnosis or misdiagnosis can be very serious for patients with SVMs.4 Impairment of spinal cord venous drainage can result in progressive neurologic deficit symptoms, such as sensory, motor, and even urogenital disturbances, which lead to disability and significantly impact the patient’s quality of life.18⇓-20 If misdiagnosed as a demyelinating disease, treatment with hormone shock therapy may lead to hematomyelia, which can be fatal.21,22 Therefore, improving the diagnostic sensitivity of pretreatment patient screening can reduce potentially serious medical risks. We recommend that the following patients should undergo CTA examination with our SSBBF-CTA method before treatment after balancing radiation and clinical needs: 1) those presenting with special neurologic symptoms, 2) those with an initial MRI suggesting evident flow void signals adjacent to the spinal cord, 3) those with existing examinations that could not definitively rule out vascular anomalies, and 4) those with contraindications for MR imaging and no contraindications for CTA.
This study achieved clear visualization and localization of SVM lesions by innovatively combining the advantages of Siemens and GE Healthcare postprocessing workstations for image postprocessing without the need for third party software. The spinal artery, a third-order or higher branch with a small diameter, runs through the intervertebral foramen and spinal canal and is closely related to the vertebrae.23 These unique anatomic features make it challenging to maintain vessel continuity while accurately subtracting the bones. According to our clinical experience, the bone subtraction algorithm of the Siemens workstation is more precise,24 but it falls short of displaying the small vessels of SVMs. The GE Healthcare workstation can display complete SVMs lesion details by tracking small vessels; however, it cannot obtain clean aorta and intercostal artery 3D-VR images using its bone subtraction algorithm. Thus, a combination of the advantages of both workstations provided clear and unobstructed 3D-VR reconstruction images of the SVMs. The fusion of a reduced-opacity bone background with clear vessels was implemented to achieve accurate localization of the SVM lesion without obstructing their visibility. A spinal CTA acquisition (from the beginning of the noncontrast scan to the completion of the CTA) rarely exceeds 1 minute and, therefore, rarely produces motion artifacts. Because the positioning coordinates of the images in the plain scan and APs are consistent and the image superposition is based on the coordinates, no additional artifacts will affect the image quality. Furthermore, junior physicians can achieve a level of accuracy in SSBBF-CTA images comparable with that of experienced physicians through short-term training, and the difference in the amount of time required to perform postprocessing was minimal. However, in complex cases, it is advisable to perform these procedures under the supervision of experienced physicians.
Preoperative information regarding the nidi/fistulas, feeding arteries, and drainage veins of SVMs is crucial for guiding the selection of clinical treatment plans. When using MPR-CTA, the less experienced physicians tended to have a lower accuracy than the physicians with more extensive experience, and both physicians demonstrated high accuracy in evaluating SVM lesions when using SSBBF-CTA. This finding indicates that the use of the SSBBF-CTA 3D-VR reconstruction technique enables the accurate identification of the key lesions of SVMs by less-experienced radiologists and clinical physicians with limited radiologic experience. Furthermore, SSBBF-CTA can significantly shorten the diagnostic time without compromising diagnostic accuracy for both junior and senior radiologists. These aspects contribute to the establishment of effective communication between the clinical and radiology departments, thereby improving diagnostic efficiency.
The advantages of CTA have yet to be fully explored and improved. Several studies have reported that 320-layer and 640-layer spiral CTA can achieve an accuracy rate of 62.5%–85.7% in locating the fistula of spinal AVFs.12,13,25 Our research aimed to update the postprocessing image quality on the basis of standard CTA, producing a more intuitive and clearer visualization of lesions and allowing a detailed and efficient analysis of lesion features of SVMs. 3D-VR images of types 3 and 4 were considered clinically acceptable diagnostic results, accounting for nearly 100% of the cases. The current research indicates that the accuracy of CE-MRA in locating fistulas for AVFs is higher than 80%,26 while time-resolved CE-MRA has an even higher accuracy rate of up to 91%.11 Therefore, in clinical practice, a reasonable selection should be made on the basis of the individual patient and hardware conditions of different hospitals, considering the respective advantages of CTA and MRA.
In addition, the classification of SVMs is complex, and at least 5 classification methods are currently known.27 Regardless of the classification standard, there are great advantages for extramedullary high-flow lesions, such as lesions classified as type I (dural AVF) and type IV (perimedullary AVF). For intramedullary lesions (type II, intramedullary glomus AVM and type III, intramedullary juvenile AVM), CTA can also provide useful information on vascular lesions, but it is limited in the evaluation of the spinal cord. For type V, extradural AVF, it may be difficult to visualize a fistula (too closely related to the bones). Challenges remain for lesions with slow flow; however, some abnormal vascular manifestations can suggest the diagnosis of SVMs.28 A second, late arterial CTA scan can also solve a part of this problem; however, the radiation dose issue needs to be considered.
This study has some limitations. By using SSBBF-CTA for comprehensive preoperative assessment of SVMs, clinicians can obtain more lesion details to develop appropriate surgical strategies, which can potentially shorten the surgical duration, reduce contrast agent use, and limit radiation exposure. However, the assumption that CTA might indirectly enhance surgical outcomes remains speculative and warrants further longitudinal observation. Although the SSBBF-CTA postprocessing technology itself does not add additional radiation, CTA examinations still need to be reasonably selected by balancing radiation and patient conditions. In addition, because of the low incidence rate of the disease, the number of included patients was relatively insufficient, and this study explored only the universal applicability of SSBBF-CTA for SVMs. Our team is continuing to collect cases for a more detailed classification to further explore the practicality of SSBBF-CTA. This research methodology has been integrated into the general work of our hospital and has already helped avoid many medical risks. A one-stop image postprocessing reconstruction software that can combine the advantages of algorithms from 2 different postprocessing workstations will make clinical work more convenient. The rapid advancement of artificial intelligence technology holds great potential for achieving simplified and increasingly accurate CTA reconstruction images in the future.
CONCLUSIONS
The SSBBF-CTA technique demonstrated excellent reproducibility, significantly enhancing both the accuracy and efficiency of the diagnosis and assessment of SVMs, with particular benefits for junior radiologists. It has the potential for substantial clinical benefits in the preoperative evaluation and selection of appropriate treatment strategies.
Footnotes
Xuehan Hu and Zhidong Yuan contributed equally to this work and should be considered co-first authors.
This work was supported by the China Postdoctoral Science Foundation (No. 2021M703373) and the Shenzhen High-Level Hospital Construction Fund.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received August 26, 2023.
- Accepted after revision December 2, 2023.
- © 2024 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.